Impact Factor ISSN: 1449-1907

 Global reach, higher impact
Global reach, higher impactTable of Content Editorial Guest Editor's Editorial: Advances in Managing Hepatitis C Virus (HCV) Infection (A Special Issue) Review Molecular Virology of Hepatitis C Virus (HCV): 2006 Update Hepatitis C Virus Serologic and Virologic Tests and Clinical Diagnosis of HCV-Related Liver Disease Epidemiology of Hepatitis C Virus (HCV) Infection The Natural History of Hepatitis C Virus (HCV) Infection Hepatitis C Virus (HCV) Infection and Hepatic Steatosis Hepatitis B Virus (HBV) and Hepatitis C Virus (HCV) Dual Infection A Practical Approach to Managing Patients with HCV Infection Treatment of Chronic HCV Infection in Special Populations Antiviral therapy of HCV in the cirrhotic and transplant candidate Management of HCV Infection and Liver Transplantation
|
Int J Med Sci Vol. 3(2) ©Ivyspring International Publisher
Special issue on virology and clinical advances of HCV infection
Guest editor: Dr. Ke-Qin Hu
Editorial: Advances in Managing Hepatitis C Virus (HCV) Infection
Ke-Qin Hu![]()
Chronic infection of hepatitis C virus (HCV) affects approximately 170 million people worldwide and 4-5 million people in the Unites States. Studies have projected a substantial burden from HCV disease and related complications, including liver failure and hepatocellular carcinoma (HCC), over the next 10 to 20 years. Since the identification of HCV in 1989, significant advances have been made in our understanding of HCV virology, diagnosis, natural history, and treatment of chronic HCV infection. The goal of this special issue of International Journal of Medical Sciences is to report and update our current knowledge in the selected areas. [Full text]
Molecular Virology of Hepatitis C Virus (HCV): 2006 Update
Volker Brass, Darius Moradpour, Hubert E. Blum ![]()
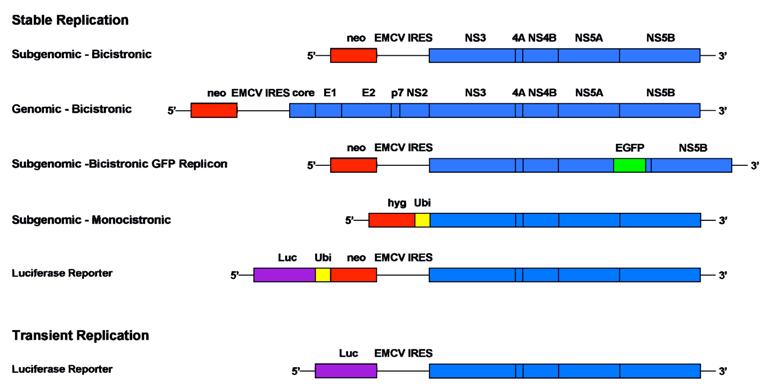
Fascinating progress in the understanding of the molecular biology of hepatitis C virus (HCV) was achieved recently. The replicon system revolutionized the investigation of HCV RNA replication and facilitated drug discovery. Novel systems for functional analyses of the HCV glycoproteins allowed the validation of HCV receptor candidates and the investigation of cell entry mechanisms. Most recently, recombinant infectious HCV could be produced in cell culture, rendering all steps of the viral life cycle, including entry and release of viral particles, amenable to systematic analysis. In this review, we summarize recent advances and discuss future research directions. [Full text]
Hepatitis C Virus Serologic and Virologic Tests and Clinical Diagnosis of HCV-Related Liver Disease
Stéphane Chevaliez, Jean-Michel Pawlotsky ![]()
The use of serological and virological tests has become essential in the management of hepatitis C virus (HCV) infection in order to diagnose infection, guide treatment decisions and assess the virological response to antiviral therapy. Virological tools include serological assays for anti-HCV antibody detection and serological determination of the HCV genotype, and molecular assays that detect and quantify HCV RNA and determine the HCV genotype. Anti-HCV antibody testing and HCV RNA testing are used to diagnose acute and chronic hepatitis C. Only patients with detectable HCV RNA should be considered for pegylated interferon alfa and ribavirin therapy and the HCV genotype should be systematically determined before treatment, as it determines the indication, the duration of treatment, the dose of ribavirin and the virological monitoring procedure. HCV RNA monitoring during therapy is used to tailor treatment duration in HCV genotype 1 infection, and molecular assays are used to assess the end-of-treatment and, most importantly the sustained virological response, i.e. the endpoint of therapy. [Full text]
Epidemiology of Hepatitis C Virus (HCV) Infection
Theodore Sy, M. Mazen Jamal ![]()
Hepatitis C virus remains a large health care burden to the world. Incidence rates across the world fluctuate and are difficult to calculate given the asymptomatic, often latent nature of the disease prior to clinical presentation. Prevalence rates across the world have changed as well with more countries aware of transfusion-related hepatitis C and more and more evidence supporting intravenous drug use as the leading risk factor of spread of the virus. This article reviews current hepatitis C virus prevalence and genotype data and examines the different risk factors associated with the virus. [Full text]
The Natural History of Hepatitis C Virus (HCV) Infection
Stephen L. Chen, Timothy R. Morgan ![]()
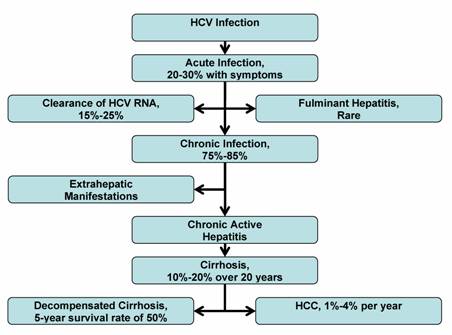
Hepatitis C virus (HCV) is a leading cause of chronic liver disease, cirrhosis, and hepatocellular carcinoma, as well as the most common indication for liver transplantation in many countries. Although the incidence of hepatitis C infection has dramatically decreased during the past decade, the worldwide reservoir of chronically infected persons is estimated at 170 million, or 3% of the global population. There is much controversy surrounding the natural history of hepatitis C infection. The rate of chronic HCV infection is affected by a person's age, gender, race, and viral immune response. Approximately 75%-85% of HCV-infected persons will progress to chronic HCV infection, and are at risk for the development of extrahepatic manifestations, compensated and decompensated cirrhosis, and hepatocellular carcinoma (HCC). The rate of progression to cirrhosis is highly variable, and is influenced by several factors, including the amount of alcohol consumption, age of initial HCV infection, degree of inflammation and fibrosis on liver biopsy, HIV and HBV coinfection, and comordid conditions. An estimated 10%-15% of HCV-infected persons will advance to cirrhosis within the first 20 years. Persons with cirrhosis are at increased risk of developing HCC. An understanding of the natural history of hepatitis C is essential to effectively manage, treat, and counsel individuals with HCV infection. [Full text]
Hepatitis C Virus (HCV) Infection and Hepatic Steatosis
Eugene J. Yoon, Ke-Qin Hu ![]()
There are two discrete forms of steatosis that may be found in patients infected with hepatitis C virus (HCV). Metabolic steatosis can coexist with HCV, regardless of genotype, in patients with risk factors such as obesity, hyperlipidemia, and insulin resistance. The second form of hepatic steatosis in HCV patients is a result of the direct cytopathic effect of genotype 3 viral infections. There have been proposed mechanisms for this process but it remains elusive. Both categories of steatosis tend to hasten the progression of liver fibrosis and therefore prompt recognition and management should be initiated in patients with HCV and steatosis. The authors review the current understanding of the relationship between hepatitis C infection and hepatic steatosis and discuss future research directions. [Full text]
Hepatitis B Virus (HBV) and Hepatitis C Virus (HCV) Dual Infection
Zhihua Liu, Jinlin Hou ![]()
Hepatitis B virus (HBV) and hepatitis C virus (HCV) infections account for a substantial proportion of liver diseases worldwide. Because the two hepatotropic viruses share same modes of transmission, coinfection with the two viruses is not uncommon, especially in areas with a high prevalence of HBV infection and among people at high risk for parenteral infection. Patients with dual HBV and HCV infection have more severe liver disease, and are at an increased risk for progression to hepatocellular carcinoma (HCC). Treatment of viral hepatitis due to dual HBV/HCV infection represents a challenge. [Full text]
A Practical Approach to Managing Patients with HCV Infection
Richard H. Huang, Ke-Qin Hu ![]()
Hepatitis C virus (HCV) infection is a major worldwide public health concern. It is a common cause of chronic liver disease and hepatocellular carcinoma. HCV antibody and HCV RNA testing are available diagnostic studies that offer high degree of accuracy. Current standard therapy includes a combination of pegylated interferon and ribavirin. Response rate is approximately 40% for genotype 1 and 80% for genotypes 2 and 3, respectively. Successful treatment can stop the progression of chronic liver disease, reduce the need for liver transplantation, and possibly decrease the risk for Hepatocellular carcinoma (HCC). Evaluating for potential treatment candidacy is an important initial step in the management of chronic HCV infection as not all individuals may need or qualify for the treatment. Understanding the natural history, the different diagnostic modalities, the current therapeutic options and, the treatment response and adverse effect profiles can help the practitioners better manage chronic HCV infection. [Full text]
Treatment of Chronic HCV Infection in Special Populations
John Hoefs, Vikramjit S. Aulakh ![]()
The mainstay of treatment of chronic hepatitis C is pegylated interferon combined with ribavirin and more than 50% of naïve patients will have viral cure with either 6 months (genotypes 2 and 3) or 12 months (genotypes 1,4, and 6) with the initial treatment. However, populations have been defined that respond less well to routine treatment including African Americans, immune suppressed populations, obese patients and cirrhotic patients. These types of patients are enriched in groups of patients who are non-responders to treatment. This article discusses viral kinetics that may impact treatment response, strategies to maximize treatment effectiveness in these populations and the treatment of non-responders in general. Early viral kinetics can be used to define response or non-response and these results can be used to modify subsequent treatment length and dose. [Full text]
Antiviral therapy of HCV in the cirrhotic and transplant candidate
Steven K. Herrine, Victor J. Navarro ![]()
The mainstay of treatment of chronic hepatitis C is pegylated interferon combined with ribavirin and more than 50% of naïve patients will have viral cure with either 6 months (genotypes 2 and 3) or 12 months (genotypes 1,4, and 6) with the initial treatment. However, populations have been defined that respond less well to routine treatment including African Americans, immune suppressed populations, obese patients and cirrhotic patients. These types of patients are enriched in groups of patients who are non-responders to treatment. This article discusses viral kinetics that may impact treatment response, strategies to maximize treatment effectiveness in these populations and the treatment of non-responders in general. Early viral kinetics can be used to define response or non-response and these results can be used to modify subsequent treatment length and dose. [Full text]
Management of HCV Infection and Liver Transplantation
Thomas D. Schiano, Paul Martin ![]()
Despite the improved efficacy of peginterferons, the rate of sustained virologic response is suboptimal in cirrhotic patients, relative to non-cirrhotic patients. However, the treatment of patients with compensated cirrhosis has recently been encouraged by expert panels. Interferon-based therapy may provide additional benefit by reducing the risk of hepatocellular carcinoma in cirrhotic patients as suggested in preliminary studies. Results of two ongoing prospective studies are awaited to answer the important question of the effectiveness of suppressive interferon therapy, even in the absence of sustained virologic response. Given the importance of recurrent HCV following liver transplantation, attention has been directed toward the antiviral treatment of patients with advanced liver disease. This approach needs to be pursued with caution given the potential morbidity of the therapy. Recently, a low accelerating dosage regimen has provided excellent results and is the subject of additional inquiry. [Full text]