ISSN: 1449-1907International Journal of Medical Sciences

Int J Med Sci 2011; 8(6):479-481. doi:10.7150/ijms.8.479 This issue Cite
Case Report
Spindle Cell Lipoma of the Hypopharynx
Muhammed Fatih Evcimik1 ![]() , Fazil Emre Ozkurt2, Tarik Sapci3, Ziya Bozkurt2
, Fazil Emre Ozkurt2, Tarik Sapci3, Ziya Bozkurt2
1. Istanbul Nisa Hospital Department of Otorhinolaryngology-Head & Neck Surgery, Istanbul, Turkey
2. Fatih Sultan Mehmet Training & Research Hospital, Department of Otorhinolaryngology-Head & Neck Surgery, Istanbul, Turkey
3. Istanbul Bilim University, Medical Faculty, Department of Otorhinolaryngology-Head & Neck Surgery, Istanbul, Turkey
Abstract
Objective: We report a rare case of a spindle cell lipoma with atypical clinical course.
Case report: A 51 year old female patient referred to our clinic with feeling of mass in the throat she had had for two years. The patient described difficulty in swallowing. Indirect laryngoscopy did not reveal any masses at bilateral pyriform sinuses, and the mucosa had a natural appearance. However, a mass with a stalk was detected in the side of the mouth when the patient retched. Endoscopic monitoring of the mass revealed its origin to be the left sinus pyriformis. No pathological structures could be detected in the indirect laryngoscopy taken after the patient gulped again. The mass was shown by magnetic resonance imaging to extend into the esophagus. It was removed using suspension microlaryngoscopy. Postoperative control revealed a complete healing at the excision site. Immunohistochemical examination for pathological diagnosis indicated a spindle cell lipoma.
Conclusions: Laryngeal and hypopharyngeal lipomas are rare forms of benign laryngeal neoplasms. Their asymptomatic course makes diagnosis difficult. The patient is presented here with related clinical and pathological features.
Keywords: Dysphagia, Head and Neck, Adult, Diagnosis, Spindle Cell Lipoma, Hypopharyngeal lipoma
Introduction
Lipomas are the most frequently observed soft tissue tumors in adults. They commonly occur in the neck and on the trunk, and are frequently located at the subdermal, while rarely at the dermal tissue layer. They are commonly found at the dorsal neck, nape, shoulders, and the back1. Spindle cell lipoma was first defined by Enzinger and Harley in 1975 2. It is more frequently found in men between the ages of 40-60, and is a soft tissue tumor characterized by replacement of the mature fat tissue by spindle cell proliferation2,3. Although they are mostly solitary, well-capsulated, and slow-growing, they should be pathologically differentiated from liposarcomas.
Case Report
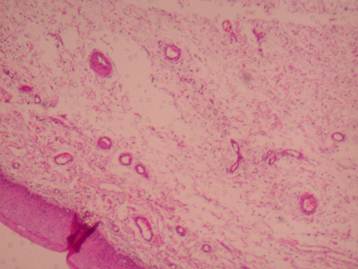
A 52-year-old female patient referred to our clinic with feeling of thickness in the throat, and a mass in the mouth while coughing. She described her complications as having begun 5 or 6 years previously, with a mass appearing in her mouth every time she retched in the last two years. The patient described no occurrence of dysphagia during this period. Her examination revealed a normal oral cavity and oropharynx. Tongue root, vallecula, sinus pyriformis, epiglottis, ventricular folds, and the vocal cords had a normal appearance upon endoscopic examination. However, it was observed that the mass projected up to her teeth when she retched (Figure 1). After the mass was stabilized, endoscopic monitoring revealed it to be smooth surfaced and its origin to be left sinus pyriformis. Preoperative magnetic resonance imaging of the patient revealed a polypoid structure approximately 6 cm long and 5 mm in diameter, corresponding to the laryngeal vestibule level in sagittal section, projecting towards the inferior from the arytenoid cartilage level. It appeared hypointense in T1-weighted sequences, and hyperintense in T2-weighted sequences. Contrast was positive following intravenous contrast administration (Figure 2). The mass was removed surgically by suspension microlaryngoscopy. The resected mass was observed to be yellowish in color; smooth-surfaced, solitary, and well-capsulated (Figure 3). Pathological examination of microscopic sections revealed a multilobular mass, with spindle and star-shaped cells lacking well-defined borders located beneath the squamous epithelium in the myxoid area. No mitosis was observed, while rare giant cells were detected (Figure 4). Angiomyxolipoma was considered initially, yet immunohistochemical analysis was requested for elimination of possible aggressive angiomyxoma and least likely low grade liposarcoma. The immunohistochemical examination revealed diffused immunoexpressions of CD34 and Vimentin. It was negative for CDK4, S-100 and MDM2. No immune expression was detected in the other panels studied. The diagnosis was confirmed as myxoid type spindle cell lipoma. The excision region was monitored as normal at postoperative month 6. The patient was asymptomatic.
Preoperative view.

Preoperative magnetic resonance imaging (Sagittal section).

Hypopharengeal mass (Intraoperative view).

Histological section of the spindle cell lipoma within collagenous stroma (Hematoxylin and Eosin X40).
Discussion
Lipomas are mesenchymal benign lesions originating from the mature lipid tissue1. They constitute approximately 0.6% of the laryngeal and hypopharyngeal benign tumors4. Laryngeal and hypopharyngeal lipomas first appeared in literature in 1995 5. Laryngeal lipomas originate from adipose tissues such as epiglottis, ventricular folds, and aryepiglottic fold. No cases with laryngeal lipoma at vocal cords have been reported. Hypopharyngeal lipomas originating from pyriform sinus have similar symptoms and pathological features with laryngeal lipogenic tumors 5. Laryngeal or hypopharyngeal lipomas are well-capsulated, smooth-surfaced, yellowish, sessile or pedicled masses. They contain histologically mature, uniform adipose cells. Spindle cell lipomas contain collagen fibers and small, cylindiric spindle cells and mixed mature adipocytes within a matrix containing mucinous material. Spindle cell lipomas appear 60 times less frequently compared to the classical lipomas 2. Described for the first time by Enzinger and Harvey in 1975, this benign tumor is characterized by replacement at varying degrees, of the mature adipose tissue by proliferation of collagen producing spindle cells 3,5,6. While the two components usually appear at equal proportions, there are lesions where one component appears dominant. Differential diagnosis may be difficult in especially cases where spindle cells are dominant. Spindle cells appear as uniform cells with single elongated nucleus, and narrow bipolar cytoplasm in SCL. Nucleolus is not prominent. Mitosis is rare. Spindle cells form short parallel clusters 3,7. Misdiagnosis is possible, as the histological characteristics of SCL are similar to those of liposarcoma 2,8; however, uniformity of the spindle cells, lack of lipoblasts, and presence of thick mature collagen fibers are typical features of SCL2. Immunohistochemically, spindle cells express CD34, bcl-2, and vimentin, but not S-100. Recently, MDM2 and CDK4, well-known key regulators of cell cycle progression, were found to be expressed in liposarcomas. They are never expressed in lipomas and normal mature adipocytes. Typical appearance of lipogenic tumors in the larynx and hypopharynx are as submucosal yellowish or polypoid masses. Adipose tissue is characterized by a less densitometric appearance compared to water at computerized tomography and magnetic resonance imaging9. SCL is generally solitary and slow-growing, and becomes symptomatic at advanced stages of life. It usually causes swallowing impairment, phonation problems, the sensation of a lump in the throat, and rarely respiratory problems due to glottic obstructions. Diagnosis is often difficult due to indistinct symptoms5,7. In this case, the feeling of a mass in the throat without dysphagia was the only symptom of large pyriform sinus lipoma. The preferred method of treatment for laryngeal and hypopharyngeal lipogenic tumors is radical endoscopic excision.
Summary
Laryngeal and hypopharyngeal lipomas are rare forms of benign laryngeal neoplasms. Their asymptomatic course makes diagnosis difficult. In this case, feeling of a mass in the throat without dysphagia was the only symptom of large pyriform sinus lipoma. Although the mass may be asymptomatic, it should be surgically removed, and undergo a detailed histopathological and immunohistochemical examination for diagnostical purposes.
Conflict of Interest
The authors have declared that no conflict of interest exists.
References
1. Rydholm A, Berg NO. Size, site and clinical incidence of lipoma. Factors in the differential diagnosis of lipoma and sarcoma. Acta Orthop Scand. 1983;54:929-934
2. Erzinger FM, Harvey DA. Spindle cell lipoma. Cancer. 1975;36:1853-1859
3. Weiss SW, Goldblum JR. Benign lipomatous tumors. In: (ed.) Weiss SW, Goldblum JR. Enzinger and Weiss's Soft Tissue Tumors; 4th ed. St Louis: Mosby. 2001:571-639
4. Jones SR, Myers EN, Barnes L. Benign neoplasms of the larynx. Otolaryngol Clin North Am. 1984;17:151-178
5. Wenig BM. Lipomas of the larynx and hypopharynx: a review of the literature with the additional of three cases. J Laryngol Otol. 1995;109:353-357
6. Persaud RAP, Kotnis R, Ong CC, Bowdler DA. A rare case of a pedunculated lipoma in the pharynx. Emerg Med J. 2002;19:275
7. Fletcher CD, Martin-Bates E. Spindle cell lipoma: A clinicopathological study with some original observations. Histopathology. 1987;11:803-817
8. Wenig BM, Weiss SW, Gnepp DR. Laryngeal and hypopharyngeal liposarcoma. A clinicopathologic study of 10 cases with a comparison to soft-tissue counterparts. Am J Surg Pathol. 1990;14:134-141
9. Remacle M, Mazy G, Marbaix E, Dooms G, Hamoir M, Van den Eeckhaut J. Contribution by tomodensitometry to the understanding and diagnosis of benign non-epithelial endolaryngeal tumours. In connection with a case of chondroma, one of lipoma and one of rhabdomyoma. Acta Otorhinolaryngol Belg. 1983;37:820-829
Author contact
![]() Corresponding author: Muhammed Fatih Evcimik, MD, Address: Istanbul Nisa Hospital, Fatih Cad. No:1 Yenibosna, Bahcelievler İstanbul, Turkey. E-mail: evcimikcom; Phone: +90 5057763567; Fax: +90 2125714564
Corresponding author: Muhammed Fatih Evcimik, MD, Address: Istanbul Nisa Hospital, Fatih Cad. No:1 Yenibosna, Bahcelievler İstanbul, Turkey. E-mail: evcimikcom; Phone: +90 5057763567; Fax: +90 2125714564
Received 2010-11-24
Accepted 2011-7-25
Published 2011-8-6