Impact Factor ISSN: 1449-1907
- Issue 9; 2026
- Issue 8; 2026
- Issue 7; 2026
- Issue 6; 2026
- Issue 5; 2026
- Volume 23; 2026
- Past Issues
- Editorial Board
- Cover Images
- Index & Coverage
- Cover Suggestion
- Special Issues
Introduction
Materials and Methods
Results
Discussion
Study Limitations
Conclusions
Acknowledgements
References

 Global reach, higher impact
Global reach, higher impactInt J Med Sci 2021; 18(1):276-283. doi:10.7150/ijms.49018 This issue Cite
Research Paper
Using CHADS2, R2CHADS2, CHA2DS2-VASc score for mortality prediction in patients with abnormal low and high ankle-brachial index
Nai-Yu Chi1,4, Ho-Ming Su1,2,3, Wen-Hsien Lee1,2,3, Wei-Chung Tsai1,2, Ying-Chih Chen1,3, Tzu-Chieh Lin1,4, Ye-Hsu Lu1, Chee-Siong Lee1,2, Tsung-Hsien Lin1,2, Wen-Ter Lai1,2, Sheng-Hsiung Sheu1,2, Po-Chao Hsu1,2 ![]()
1. Division of Cardiology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan.
2. Faculty of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan.
3. Department of Internal Medicine, Kaohsiung Municipal Siaogang Hospital, Kaohsiung, Taiwan.
4. Department of Internal Medicine, Kaohsiung Municipal Ta-Tung Hospital, Kaohsiung, Taiwan.
Received 2020-6-2; Accepted 2020-11-2; Published 2021-1-1
Abstract
Abnormal low and high ankle brachial index (ABI) is regarded as peripheral artery disease (PAD) which has extremely high morbidity and mortality. How to identify high-risk PAD patients with increased mortality is very important to improve the outcome. CHADS2, R2CHADS2, and CHA2DS2-VASc score are clinically useful scores to evaluate the annual risk of stroke in patients with atrial fibrillation. However, there was no literature discussing the usefulness of these scores for cardiovascular (CV) and all-cause mortality prediction in the patients with abnormal ABI. This longitudinal study enrolled 195 patients with abnormal low (< 0.9) and high ABI (> 1.3). CHADS2, R2CHADS2, and CHA2DS2-VASc score were calculated for each patient. CV and all-cause mortality data were collected for outcome prediction. The median follow-up to mortality was 90 months. After multivariate analysis, CHADS2, R2CHADS2, and CHA2DS2-VASc score were significant predictors of CV and all-cause mortality (all P < 0.001). CHA2DS2-VASc score had a better additive predictive value than CHADS2 and R2CHADS2 score for CV mortality prediction. R2CHADS2 and CHA2DS2-VASc score had better additive predictive values than CHADS2 score for all-cause mortality prediction. In conclusion, our study is the first study to investigate the usefulness of CHADS2, R2CHADS2, and CHA2DS2-VASc score for mortality prediction in patients with abnormal ABI. Our study showed all three scores are significant predictors for CV and all-cause mortality although there are some differences between the scores. Therefore, using the three scoring systems may help physicians to identify the high-risk PAD patients with increased mortality.
Keywords: all-cause mortality, cardiovascular mortality, CHADS2 score, CHA2DS2-VASc score, chronic kidney disease, R2CHADS2 score
Introduction
Ankle-brachial index (ABI) is a simple and reliable diagnostic tool for peripheral arterial disease (PAD) [1,2]. ABI of each leg is calculated by the ratio of the ankle over the higher brachial systolic blood pressure [3]. ABI < 0.9 is not only established as a diagnostic method for PAD, but also a strong predictor for cardiovascular (CV) and all-cause mortality [4-6]. In addition, ABI > 1.3 is also considered as abnormal and suggests hardening or calcification of the incompressible vessel walls, which reflects another form of PAD [7-10].
CHADS2, R2CHADS2, and CHA2DS2-VASc score are all useful scoring systems to evaluate the risk of stroke in patients with atrial fibrillation (AF) [11-16]. In AF patients, there is a significant association between the CHADS2, R2CHADS2, and CHA2DS2-VASc score and the annual risk of stroke. Furthermore, these scoring systems were recently used to predict CV outcomes in the patients without AF [17-25]. However, there was no literature discussing about the usefulness of CHADS2, R2CHADS2 and CHA2DS2-VASc score for CV and all-cause mortality prediction in the patients with abnormal low and high ABI. Therefore, we conducted this study to evaluate the issue.
Materials and Methods
Study population
Study population was enrolled from a group of patients arranged for examinations of echocardiography at Kaohsiung Municipal Siaogang Hospital from March 2010 to March 2012 because of suspecting hypertension, coronary artery disease, heart failure, and abnormal cardiac physical examination, and survey for dyspnea. Patients with abnormal low and high ABI defined as ABI < 0.9 or ABI > 1.3 were included. We excluded the subjects with significant atrial fibrillation, diseases of mitral and aortic valve. Finally, 195 patients were included in our study.
Ethics Statement
Our study protocol was approved by the institutional review board committee of the Kaohsiung Medical University Hospital (KMUH-IRB). Informed consents have obtained from the patients and our study was conducted according to the principles expressed in the Declaration of Helsinki.
Assessment of ABI
The values of ABI were measured by using an ABI-form device (VP1000; Colin Co. Ltd., Komaki, Japan), which automatically and simultaneously measures blood pressures in both arms and ankles using an oscillometric method [26]. ABI of each leg was calculated by the ratio of the ankle over the higher brachial systolic blood pressure. After obtaining bilateral ABIs, the lower one was selected for later analysis.
Calculation of CHADS2, R2CHADS2, and CHA2DS2-VASc score
CHADS2 score was calculated for each patient based on a scoring system in which 2 points were assigned for a history of stroke or transient ischemic attack and 1 point was assigned for age ≥75 years, the presence of hypertension, diabetes mellitus, and congestive heart failure [11,12]. R2CHADS2 score was calculated for each patient based on a point system in which 2 points were assigned for renal dysfunction implicated by estimated glomerular filtration rate < 60 ml/min/1.73 m2 and a history of stroke, and 1 point was assigned for age ≥75 years, the presence of congestive heart failure, hypertension, and diabetes [16]. CHA2DS2-VASc score was calculated for each patient based on a point system in which 2 points were assigned for age ≥75 years and a history of stroke, and 1 point was assigned for congestive heart failure, hypertension, age between 65 and 74 years, diabetes mellitus, female sex, and vascular disease [13].
Collection of medical and demographic data
Medical data and demographic including age, gender, and other comorbid diseases were collected from medical records or interviews with patients. Hypertension was defined as systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg or anti-hypertensive drugs were prescribed. Diabetes was defined as fasting blood glucose level greater than 126 mg/dL or hypoglycemic agents were used to control blood glucose levels. Dyslipidemia was defined as total cholesterol > 200 mg/dL, low density lipoprotein > 130 mg/dL, or triglycerides > 200 mg/dL. Information about patient medications including aspirin, angiotensin converting enzyme inhibitors, angiotensin II receptor blockers, β-blockers, calcium channel blockers, diuretics, and statin at enrollment was obtained from medical records.
Definition of CV and all-cause mortality
All study participants were followed up till December 2018. Survival information and causes of death were obtained from the official death certificate and final confirmation by the Ministry of Health and Welfare. The causes of death were classified by the International Classification of Diseases 9th Revision. Causes of CV mortality were defined deaths due to cerebral vascular disease, ischemic heart disease, myocardial infarction, heart failure, valvular heart disease and atherosclerotic vascular disease.
Statistical analysis
We used SPSS 22.0 software for statistical analysis. Our data was expressed as mean ± standard deviation, percentage, or median (25th-75th percentile) for follow-up period. Continuous and categorical variables between groups were compared by independent samples t test and Chi-square test, respectively. The significant variables in the univariate analysis were selected for multivariable analysis. Time to the CV and overall mortality events and covariates of risk factors were modeled using the Cox proportional hazards model with forward selection. The incremental value of CHADS2, R2CHADS2, and CHA2DS2-VASc score over conventional parameters to assess the risk for CV and all-cause mortality were studied by calculating the improvement in global chi-square. Kaplan-Meier survival plots were calculated from baseline to time of mortality events. All tests were 2-sided and the level of significance was established as P < 0.05.
Results
Among the 195 subjects, mean age was 66 ± 15 years. CHADS2, R2CHADS2, and CHA2DS2-VASc score in patients with ABI < 0.9 (n = 81) were 2.64±1.29, 4.12±1.82, and 4.27±1.60, respectively. CHADS2, R2CHADS2, and CHA2DS2-VASc score in patients with ABI > 1.3 (n = 114) were 1.42±1.03, 2.23±1.63, and 2.30±1.50, respectively. CV and overall mortality data were collected up to December 2018. Mortality data were obtained from the Collaboration Center of Health Information Application (CCHIA), Ministry of Health and Welfare, Executive Yuan, Taiwan. The follow-up period to mortality events was 90 (25th-75th percentile: 39-101) months in all patients. Mortality events were documented during the follow-up period, including CV mortality (n= 41) and all-cause mortality (n= 96).
Table 1 compares the clinical characteristics between patients with and without mortality. Compared to patients without mortality, patients with mortality were found to have an older age, higher prevalence of diabetes mellitus, higher heart rate, lower body mass index (BMI), lower estimated glomerular filtration rate, higher CHADS2, R2CHADS2, and CHA2DS2-VASc score, and higher percentage of diuretic use.
Comparison of clinical characteristics between patients with mortality and without mortality
| Baseline Characteristics | Mortality (-) | Mortality (+) | P value |
|---|---|---|---|
| Number | 99 | 96 | |
| Age (yr) | 60 ± 13 | 73 ± 13 | <0.001 |
| Male gender (%) | 71.7% | 59.4% | 0.073 |
| Smoking (%) | 15.2% | 8.3% | 0.183 |
| Diabetes (%) | 32.3% | 51.0% | 0.009 |
| Hypertension (%) | 78.6% | 85.4% | 0.264 |
| Dyslipidemia (%) | 49.3% | 42.1% | 0.475 |
| Heart rate (min-1) | 68 ± 12 | 72 ± 13 | 0.013 |
| Body mass index (kg/m2) | 27.2 ± 4.4 | 25.4 ± 4.4 | 0.005 |
| eGFR | 59.5 ± 17.6 | 40.8 ± 20.3 | <0.001 |
| CHADS2 score | 1.38 ± 1.04 | 2.49 ± 1.29 | <0.001 |
| R2CHADS2 score | 2.13 ± 1.65 | 3.93 ± 1.81 | <0.001 |
| CHA2DS2-VASc score | 2.29 ± 1.51 | 3.97 ± 1.73 | <0.001 |
| Medication | |||
| Aspirin | 43.3% | 46.1% | 0.756 |
| β-blockers | 45.5% | 35.4% | 0.189 |
| CCBs | 42.4% | 51.0% | 0.252 |
| ACEIs | 9.1% | 16.8% | 0.134 |
| ARBs | 49.5% | 57.3% | 0.316 |
| Diuretics | 30.3% | 52.1% | 0.002 |
| Statin | 45.5% | 40.6% | 0.563 |
Abbreviations: ACEI, angiotensin converting enzyme inhibitor; ARB, angiotensin II receptor blocker; CCB, calcium channel blocker; eGFR, estimated glomerular filtration rate.
Table 2 shows the predictors of CV and all-cause mortality using Cox proportional hazards model by univariate analysis. Age, hypertension, diabetes, and renal function were not included in the univariate analysis because these variables were included in the three scoring systems. For prediction of CV mortality, higher mean blood pressure, increased heart rate, lower BMI, and higher CHADS2, R2CHADS2, and CHA2DS2-VASc score (all three P < 0.001) are significant predictors. For prediction of all-cause mortality, higher mean blood pressure, increased heart rate, lower BMI, higher CHADS2, R2CHADS2, and CHA2DS2-VASc score (all P < 0.001), and diuretic use are significant predictors.
Predictors of cardiovascular events (all-cause mortality) using Cox proportional hazards model
| Parameter | Univariate (CV mortality) | Univariate (all-cause mortality) | ||
|---|---|---|---|---|
| HR (95% CI) | P | HR (95% CI) | P | |
| Male gender | 0.815 (0.398-1.668) | 0.576 | 0.691 (0.432-1.104) | 0.122 |
| Mean blood pressure (mmHg) | 1.039 (1.015-1.062) | 0.001 | 1.019 (1.003-1.036) | 0.018 |
| Dyslipidemia (Yes or No) | 1.421 (0.599-3.373) | 0.426 | 0.772 (0.452-1.320) | 0.344 |
| Smoking (ever vs no) | 0.836 (0.293-2.386) | 0.738 | 0.724 (0.347-1.510) | 0.389 |
| Heart rate (per beat/minute) | 1.039 (1.015-1.062) | 0.001 | 1.020 (1.003-1.039) | 0.023 |
| Body mass index (per kg/m2) | 0.894 (0.815-0.981) | 0.017 | 0.928 (0.876-0.984) | 0.012 |
| CHADS2 score | 1.643 (1.295-2.085) | <0.001 | 1.580 (1.347-1.854) | <0.001 |
| R2CHADS2 score | 1.479 (1.237-1.769) | <0.001 | 1.449 (1.286-1.632) | <0.001 |
| CHA2DS2-VASc score | 1.578 (1.308-1.903) | <0.001 | 1.502 (1.326-1.702) | <0.001 |
| Medications | ||||
| Aspirin use | 0.658 (0.312-1.391) | 0.273 | 1.088 (0.682-1.735) | 0.724 |
| Beta blocker use | 1.074 (0.534-2.160) | 0.841 | 0.733 (0.451-1.192) | 0.211 |
| Calcium channel blocker use | 1.329 (0.660-2.676) | 0.425 | 1.274 (0.800-2.029) | 0.308 |
| ACEI use | 1.192 (0.417-3.409) | 0.743 | 1.151 (0.572-2.315) | 0.694 |
| ARB use | 1.131 (0.562-2.276) | 0.730 | 1.368 (0.851-2.198) | 0.196 |
| Diuretic use | 1.954 (0.971-3.934) | 0.061 | 1.872 (1.175-2.982) | 0.008 |
HR: hazard ratio; CI: confidence interval; other abbreviations as in Table 1.
Table 3 shows the predictors of CV mortality using Cox proportional hazards model by multivariate analysis. All of the three models included the significant variables in the univariate analysis including mean blood pressure, heart rate, and BMI. CHADS2, R2CHADS2, and CHA2DS2-VASc score were added in model 1 to model 3, respectively. In model 1, higher mean blood pressure, increased heart rate, and higher CHADS2 score (hazard ratio [HR] = 1.632; 95% confidence interval [CI]: 1.252-2.129; P < 0.001) were significant predictors after multivariate analysis. In model 2, higher mean blood pressure, increased heart rate, lower BMI, and higher R2CHADS2 score (HR = 1.433; 95% CI: 1.181-1.739; P < 0.001) were significant predictors after multivariate analysis. In model 3, higher mean blood pressure, increased heart rate, and higher CHA2DS2-VASc score (HR = 1.639; 95% CI: 1.324-2.028; P < 0.001) were significant predictors after multivariate analysis.
Predictors of CV mortality using Cox proportional hazards model (multivariate analysis)
| Parameter | Model 1 | P | Model 2 | P | Model 3 | P |
|---|---|---|---|---|---|---|
| HR (95% CI) | HR (95% CI) | HR (95% CI) | ||||
| MBP (mmHg) | 1.038 (1.03-1.063) | 0.003 | 1.032 (1.007-1.059) | 0.013 | 1.043 (1.018-1.068) | 0.001 |
| HR (beat/min) | 1.043 (1.015-1.072) | 0.003 | 1.041 (1.012-1.070) | 0.005 | 1.050 (1.019-1.082) | 0.001 |
| BMI (kg/m2) | 0.913 (0.831-1.002) | 0.056 | 0.910 (0.829-0.999) | 0.047 | 0.925 (0.841-1.017) | 0.107 |
| CHADS2 score | 1.632 (1.252-2.129) | <0.001 | - | - | - | - |
| R2CHADS2 score | - | - | 1.433 (1.181-1.739) | <0.001 | - | - |
| CHA2DS2-VASc score | - | - | - | - | 1.639 (1.324-2.028) | <0.001 |
HR: hazard ratio; CI: confidence interval; other abbreviations as in Table 1.
Table 4 shows the predictors of all-cause mortality using Cox proportional hazards model by multivariate analysis. All of the three models included the significant variables in the univariate analysis including mean blood pressure, heart rate, BMI, and diuretic use. CHADS2, R2CHADS2, and CHA2DS2-VASc score were added in model 1 to model 3, respectively. In model 1, higher mean blood pressure, lower BMI, and higher CHADS2 score (HR = 1.512; 95% CI: 1.268-1.802; P < 0.001) were significant predictors after multivariate analysis. In model 2, lower BMI, and higher R2CHADS2 score (HR = 1.410; 95% CI: 1.238-1.606; P < 0.001) were significant predictors after multivariate analysis. In model 3, higher mean blood pressure, increased heart rate, and higher CHA2DS2-VASc score (HR = 1.480; 95% CI: 1.290-1.699; P < 0.001) were significant predictors after multivariate analysis.
Predictors of overall mortality using Cox proportional hazards model (multivariate analysis)
| Parameter | Model 1 | P | Model 2 | P | Model 3 | P |
|---|---|---|---|---|---|---|
| HR (95% CI) | HR (95% CI) | HR (95% CI) | ||||
| MBP (mmHg) | 1.019 (1.002-1.036) | 0.031 | 1.014 (0.996-1.032) | 0.119 | 1.023 (1.005-1.040) | 0.010 |
| HR (beat/min) | 1.018 (0.998-1.039) | 0.084 | 1.019 (0.998-1.040) | 0.070 | 1.020 (0.999-1.043) | 0.010 |
| BMI (kg/m2) | 0.941 (0.886-0.999) | 0.045 | 0.940 (0.886-0.997) | 0.040 | 0.953 (0.897-1.012) | 0.114 |
| Diuretic | 1.246 (0.750-2.071) | 0.396 | 1.079 (0.643-1.813) | 0.773 | 1.150 (0.694-1.907) | 0.587 |
| CHADS2 score | 1.512 (1.268-1.802) | <0.001 | - | - | - | - |
| R2CHADS2 score | - | - | 1.410 (1.238-1.606) | <0.001 | - | - |
| CHA2DS2-VASc score | - | - | - | - | 1.480 (1.290-1.699) | <0.001 |
HR: hazard ratio; CI: confidence interval; other abbreviations as in Table 1.
Figure 1 shows the Nested Cox model for CV mortality (Figure 1A) and all-cause mortality (Figure 1B). The basic model in Figure 1A were mean blood pressure, heart rate, and body mass index. After adding CHADS2, R2CHADS2, and CHA2DS2-VASc score into the basic model respectively, we found these three models had better predictive values for CV mortality than basic model itself (all three P < 0.001). In addition, basic model + CHA2DS2-VASc score had a better predictive value for CV mortality than basic model + CHADS2 score and basic model + R2CHADS2 score (P = 0.005 and P = 0.02, respectively). The basic model in Figure 1B were mean blood pressure, heart rate, body mass index, and diuretic use. After adding CHADS2, R2CHADS2, and CHA2DS2-VASc score into the basic model respectively, we found these three models had better predictive values for all-cause mortality than basic model itself (all three P < 0.001). In addition, basic model + R2CHADS2 score and basic model + CHA2DS2-VASc score had better predictive values for all-cause mortality than basic model + CHADS2 score (P = 0.01 and P = 0.001, respectively).
Nested Cox model for CV mortality (Figure 1A) and all-cause mortality (Figure 1B). Basic model in Figure 1A: mean blood pressure, heart rate, and body mass index. Basic model in Figure 1B: mean blood pressure, heart rate, body mass index, and diuretic use.
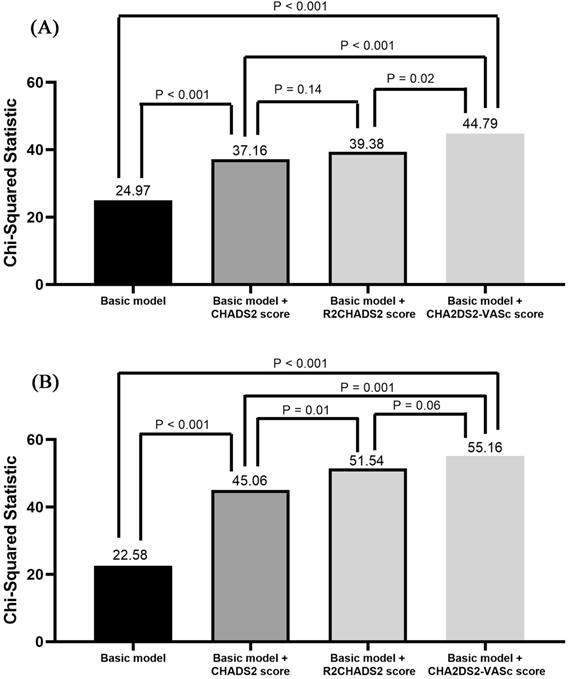
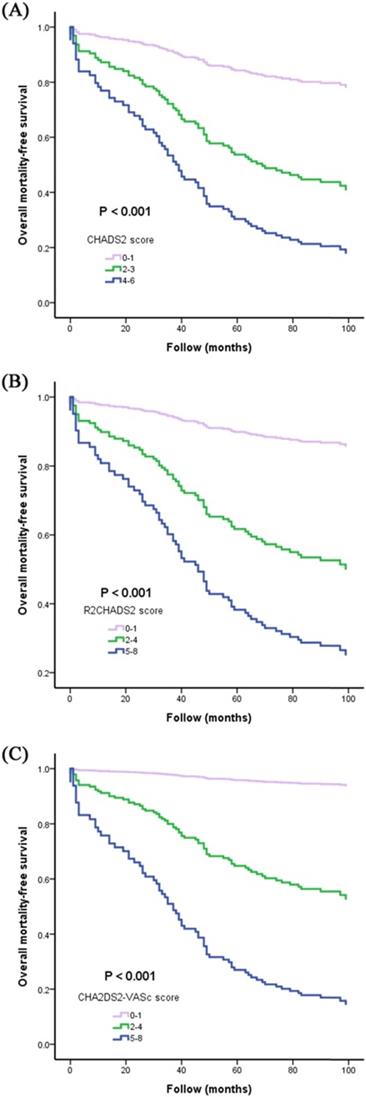
Figure 2 illustrates the Kaplan-Meier curves of CHADS2, R2CHADS2, and CHA2DS2-VASc score for all-cause mortality-free survival (all three P < 0.001).
The Kaplan-Meier curves of CHADS2, R2CHADS2, and CHA2DS2-VASc score for all-cause mortality-free survival (Figure 2A, 2B, and 2C).
Discussion
Our study was aimed to investigate the usefulness of CHADS2, R2CHADS2, and CHA2DS2-VASc score on the prediction of CV and all-cause mortality in patients with abnormal low and high ABI. There were several major findings in this study. First, CHADS2, R2CHADS2, and CHA2DS2-VASc score were significant predictors of CV and all-cause mortality after multivariate analysis. Second, CHADS2, R2CHADS2, and CHA2DS2-VASc score had additive predictive values than conventional parameters for prediction of CV and all-cause mortality. Third, basic model + CHA2DS2-VASc score had a better predictive value for CV mortality than basic model + CHADS2 score and basic model + R2CHADS2 score. Fourth, basic model + R2CHADS2 score and basic model + CHA2DS2-VASc score had better predictive values for all-cause mortality than basic model + CHADS2 score.
Abnormal low and high ABI are not only regarded as diagnostic parameters of PAD, but also strong predictors of CV and all-cause mortality [4-10]. PAD is a systemic atherosclerotic disease with similar risk factors as cerebrovascular disease and coronary artery disease (CAD) [27]. Risk factors for PAD include advanced age, hypertension, diabetes mellitus, dyslipidemia, cigarette smoking, races, chronic kidney disease, and so on [27,28]. Patients with PAD had extremely high morbidity and mortality [29,30]. 5-year mortality of patients with symptomatic and asymptomatic PAOD is 24% and 19% [29]. However, mortality could be as high as 20% within 6 months from diagnosis and exceeding 50% at 5 years for the patients with critical limb ischemia [30]. Therefore, how to identify high risk PAD patients with increased mortality become extremely important.
CHADS2, R2CHADS2, and CHA2DS2-VASc score are all simple and useful scoring system to evaluate the risk of stroke in AF patients [11-16]. However, R2CHADS2 score and CHA2DS2-VASc score have recently become more useful scores and outperformed CHADS2 score for prediction of stroke and systemic embolization [13,16]. In addition, all three scores were used to predict CV outcomes and mortality in non-AF patients [17-25]. Li Y et al. used CHADS2 and R2CHADS2 score to predict long-term outcome for CAD patients and their data showed both of scores are useful tools in predicting long-term outcome [22]. Hoshino T et al. investigated CHADS2, R2CHADS2, and CHA2DS2-VASc score for prediction of 3-month functional outcome of stroke in patients with prior CAD and they found all three scores are useful scoring systems for predicting the outcomes [21]. Chen YL et al. evaluated CHADS2, R2CHADS2, and CHA2DS2-VASc scores for prediction of 1-year all-cause mortality for patients with systolic heart failure and results showed all three scores can be used to predict the mortality; however, R2CHADS2 score is more accurate than CHADS2 and CHA2DS2-VASc score [20]. Furthermore, these three scoring systems were also reported to be useful tools for predicting outcomes in patients with acute coronary syndrome, syncope, sick sinus syndrome, heart failure, and so on [19,23-25]. However, there was no literature investigating the usefulness of CHADS2, R2CHADS2, and CHA2DS2-VASc score for CV and all-cause mortality prediction in the patients with abnormal low and high ABI. Our study is the first study to discuss the issue.
In our study, all of CHADS2, R2CHADS2, and CHA2DS2-VASc score were associated with increased CV and all-cause mortality in univariate and multivariate analysis. In addition, although all three scores had additive predictive values than conventional parameters for prediction of CV and all-cause mortality, CHA2DS2-VASc score had a better predictive value than CHADS2 and R2CHADS2 score for prediction of CV mortality in direct comparison of multivariate model (P = 0.005 and 0.02, respectively). R2CHADS2 and CHA2DS2-VASc score also had better predictive values than CHADS2 score for prediction of all-cause mortality in direct comparison of multivariate model (P = 0.01 and 0.001, respectively).
Study Limitations
First, our study was aimed to investigate the mortality outcome, so non-fatal outcomes were not evaluated. Second, the majority of our patients were treated with CV medications. For ethical reasons, we did not withdraw these medications. Hence, we could not exclude the influence of CV medications on our study. However, we already adjusted the associated usage of CV medications in multivariate analysis, which can reduce the influence of medication.
Conclusions
Our study is the first study to investigate the usefulness of CHADS2, R2CHADS2, and CHA2DS2-VASc score in patients with abnormal low and high ABI for prediction of long-term CV and all-cause mortality. Our study showed all three scores are significant predictors for long-term CV and all-cause mortality. In addition, CHA2DS2-VASc score had a better predictive value than CHADS2 and R2CHADS2 score for CV mortality, and R2CHADS2 and CHA2DS2-VASc score had better predictive values than CHADS2 score for all-cause mortality in direct comparison of multivariate model. Therefore, using CHADS2, R2CHADS2, and CHA2DS2-VASc score to screen patients with abnormal low and high ABI can help physicians to identify the high-risk PAD patients with increased mortality.
Acknowledgements
Mortality data were provided by the Collaboration Center of Health Information Application, Ministry of Health and Welfare, Executive Yuan. The research presented in this article is supported by the grants from the Kaohsiung Medical University Hospital (KMUH97-7G36), Kaohsiung Medical University, Kaohsiung, Taiwan.
Competing Interests
The authors have declared that no competing interest exists.
References
1. Fowkes FG, Housley E, Cawood EH. et al. Edinburgh Artery Study: prevalence of asymptomatic and symptomatic peripheral arterial disease in the general population. Int J Epidemiol. 1991;20(2):384-392
2. Hasimu B, Li J, Nakayama T. et al. Ankle brachial index as a marker of atherosclerosis in Chinese patients with high cardiovascular risk. Hypertens Res. 2006;29(1):23-28
3. Aboyans V, Ricco JB, Bartelink MEL. et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: the European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur Heart J. 2018;39(9):763-816
4. Chen SC, Chang JM, Hwang SJ. et al. Ankle brachial index as a predictor for mortality in patients with chronic kidney disease and undergoing haemodialysis. Nephrology (Carlton). 2010;15(3):294-299
5. Heald CL, Fowkes FG, Murray GD. et al. Risk of mortality and cardiovascular disease associated with the ankle-brachial index: Systematic review. Atherosclerosis. 2006;189(1):61-69
6. Hanssen NM, Huijberts MS, Schalkwijk CG. et al. Associations between the ankle-brachial index and cardiovascular and all-cause mortality are similar in individuals without and with type 2 diabetes: nineteen-year follow-up of a population-based cohort study. Diabetes Care. 2012;35(8):1731-1735
7. Adragao T, Pires A, Branco P. et al. Ankle-brachial index, vascular calcifications and mortality in dialysis patients. Nephrol Dial Transplant. 2012;27(1):318-325
8. Singh PP, Abbott JD, Lombardero MS. et al. The prevalence and predictors of an abnormal ankle-brachial index in the Bypass Angioplasty Revascularization Investigation 2 Diabetes (BARI 2D) trial. Diabetes Care. 2011;34(2):464-467
9. Arain FA, Ye Z, Bailey KR. et al. Survival in patients with poorly compressible leg arteries. J Am Coll Cardiol. 2012;59(4):400-407
10. Aboyans V, Desormais I, Lacroix P. Poorly compressible leg arteries: a specific presentation of peripheral artery disease. J Am Coll Cardiol. 2012;60(7):643 author reply 643-644
11. Gage BF, Waterman AD, Shannon W. et al. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA. 2001;285(22):2864-2870
12. Gage BF, van Walraven C, Pearce L. et al. Selecting patients with atrial fibrillation for anticoagulation: stroke risk stratification in patients taking aspirin. Circulation. 2004;110(16):2287-2292
13. Lip GY, Nieuwlaat R, Pisters R. et al. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137(2):263-272
14. Kirchhof P, Benussi S, Kotecha D. et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37(38):2893-2962
15. January CT, Wann LS, Calkins H. et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2019;74(1):104-132
16. Piccini JP, Stevens SR, Chang Y. et al. Renal dysfunction as a predictor of stroke and systemic embolism in patients with nonvalvular atrial fibrillation: validation of the R(2)CHADS(2) index in the ROCKET AF (Rivaroxaban Once-daily, oral, direct factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation) and ATRIA (AnTicoagulation and Risk factors In Atrial fibrillation) study cohorts. Circulation. 2013;127(2):224-232
17. Chao TF, Liu CJ, Chen SJ. et al. CHADS2 score and risk of new-onset atrial fibrillation: a nationwide cohort study in Taiwan. Int J Cardiol. 2013;168(2):1360-1363
18. Welles CC, Whooley MA, Na B. et al. The CHADS2 score predicts ischemic stroke in the absence of atrial fibrillation among subjects with coronary heart disease: data from the Heart and Soul Study. Am Heart J. 2011;162(3):555-561
19. Poci D, Hartford M, Karlsson T. et al. Role of the CHADS2 score in acute coronary syndromes: risk of subsequent death or stroke in patients with and without atrial fibrillation. Chest. 2012;141(6):1431-1440
20. Chen YL, Cheng CL, Huang JL. et al. Mortality prediction using CHADS2/CHA2DS2-VASc/R2CHADS2 scores in systolic heart failure patients with or without atrial fibrillation. Medicine (Baltimore). 2017;96(43):e8338
21. Hoshino T, Ishizuka K, Shimizu S. et al. CHADS2, CHA2DS2-VASc, and R2CHADS2 scores are associated with 3-month functional outcome of stroke in patients with prior coronary artery disease. Circ J. 2014;78(6):1481-1485
22. Li Y, Wang J, Lv L. et al. Usefulness of the CHADS2 and R2CHADS2 scores for prognostic stratification in patients with coronary artery disease. Clin Interv Aging. 2018;13:565-571
23. Ruwald MH, Ruwald AC, Jons C. et al. Evaluation of the CHADS2 risk score on short- and long-term all-cause and cardiovascular mortality after syncope. Clin Cardiol. 2013;36(5):262-268
24. Svendsen JH, Nielsen JC, Darkner S. et al. CHADS2 and CHA2DS2-VASc score to assess risk of stroke and death in patients paced for sick sinus syndrome. Heart. 2013;99(12):843-848
25. Paoletti Perini A, Bartolini S, Pieragnoli P. et al. CHADS2 and CHA2DS2-VASc scores to predict morbidity and mortality in heart failure patients candidates to cardiac resynchronization therapy. Europace. 2014;16(1):71-80
26. Yamashina A, Tomiyama H, Takeda K. et al. Validity, reproducibility, and clinical significance of noninvasive brachial-ankle pulse wave velocity measurement. Hypertens Res. 2002;25(3):359-364
27. Bartholomew JR, Olin JW. Pathophysiology of peripheral arterial disease and risk factors for its development. Cleve Clin J Med. 2006;73(Suppl 4):S8-14
28. Selvin E, Erlinger TP. Prevalence of and risk factors for peripheral arterial disease in the United States: results from the National Health and Nutrition Examination Survey, 1999-2000. Circulation. 2004;110(6):738-743
29. Diehm C, Allenberg JR, Pittrow D. et al. Mortality and vascular morbidity in older adults with asymptomatic versus symptomatic peripheral artery disease. Circulation. 2009;120(21):2053-2061
30. Abu Dabrh AM, Steffen MW, Undavalli C. et al. The natural history of untreated severe or critical limb ischemia. J Vasc Surg. 2015;62(6):1642-1651 e1643
Author contact
![]() Corresponding author: Po-Chao Hsu, MD, PhD, Division of Cardiology, Department of Internal Medicine; Kaohsiung Medical University Hospital, 100 Tzyou 1st Road, Kaohsiung. 80708, Taiwan, ROC. Tel: +886-7-3121101 ext 7738/Fax: +886-7-3234845/E-mail: pochao.hsucom.
Corresponding author: Po-Chao Hsu, MD, PhD, Division of Cardiology, Department of Internal Medicine; Kaohsiung Medical University Hospital, 100 Tzyou 1st Road, Kaohsiung. 80708, Taiwan, ROC. Tel: +886-7-3121101 ext 7738/Fax: +886-7-3234845/E-mail: pochao.hsucom.