Impact Factor ISSN: 1449-1907

 Global reach, higher impact
Global reach, higher impactInt J Med Sci 2011; 8(1):9-15. doi:10.7150/ijms.8.9 This issue Cite
Research Paper
Experimental ablation of the pancreas with high intensity focused ultrasound (HIFU) in a porcine model
Biao Xie, Yu-Yuan Li, Lin Jia ![]() , Yu-Qiang Nie, Hong Du, Shu-Man Jiang
, Yu-Qiang Nie, Hong Du, Shu-Man Jiang
Department of Gastroenterology, Guangzhou First Municipal People's Hospital, Guangzhou Nan Sha Center Hospital Affiliated to Guangzhou Medical College, Guangzhou, Guangdong Province 510180, China
Received 2010-9-29; Accepted 2010-12-8; Published 2010-12-17
Abstract
The aim of this study was to determine the feasibility and safety of high intensity focused ultrasound's (HIFU) in pancreatic diseases. Twelve pigs were divided into three groups. The pancreases of pigs in Group A were ablated directly with HIFU, but those in Group B and C ablated by extracorporeal HIFU. The pigs in Group C were sacrificed at day 7 after HIFU. Serological parameters were determined pre-operation and post-operation. The entire pancreas was removed for histological examination. Each animal tolerate the HIFU ablation well. The complete necrosis was observed in targeted regions. The margins of the necrotic regions were clearly delineated from the surrounding normal tissues. Infiltration of inflammatory cells and phorocytosis on the boundary were found in group C. Blood and urine amylase levels were relatively steady after HIFU. No acute pancreatitis or severe complications occurred. In conclusion, HIFU ablation on the pancreas was safe and effective in experimental pigs.
Keywords: High intensity focused ultrasound, Pancreas, Ablation.
INTRODUCTION
Pancreatic cancer is one of the most common malignancies of the digestive system and has poor prognosis. The incidence of pancreatic cancer is gradually increasing worldwide [1]. Currently, surgical intervention remains the only potential curative therapy; however, the majority of pancreatic cancers are not suitable for surgical resection due to the advanced stage. Therefore, non-operative therapies are alternatives for patients with pancreatic cancer at the advanced stage [2].
High intensity focused ultrasound (HIFU) is a minimally invasive technique for the regional treatment of solid tumors. It can transmit external acoustic energy into the body and selectively produce target lesions without damaging the intervening tissues. Lynn et al first applied HIFU in animal study in 1942 [3]. During the 1950s and 1960s, numerous studies have been conducted to investigate the role of HIFU in treating human neurological disorders [2, 4]. At the same time, the characteristics of HIFU and its effects on experimental tumors have also been explored. In Europe and Japan, HIFU has been used in the clinical treatment of prostate hypertrophy. In 1956, HIFU was first introduced to the treatment of human solid carcinomas [4]. The treatment of hepatocellular carcinoma (HCC) with HIFU was approved in China in 1999 and is currently being performed in many centers [5, 6]. To date, HIFU has been used to treat many tumours of solid organs including HCC, renal carcinoma, sarcomas, urinary bladder tumors and prostate carcinoma [7-10]. Some nonrandomized studies using HIFU for the palliative treatment of advanced pancreatic cancer (prolongation of life and relief of carcinoma-related pain) have been reported [11, 12]. Because pancreatic injury may result in severe pancreatitis and other serious complications, the safety of HIFU is an important concern. Only a few experimental data have been reported with pathologic evidence for its efficacy and safety. To evaluate the relationship between HIFU energy and pancreas histology, a preclinical in vivo study was conducted in swine demonstrating the feasibility and safety of HIFU for pancreas ablation [13]. In the present study, we aimed to confirm the feasibility and safety of HIFU ablation to the pancreas of pigs using microscopy to provide additional evidence to support its clinical application.
MATERIALS AND METHODS
Animals
Twelve mongrel pigs (both sexes) weighing 24-26 kg were purchased from the Animal Center of Guangzhou Medical College (Guangzhou City, Guangdong Province, China). The pigs were divided randomly into three groups (n = 4 per group). In the Group A, laparotomy was performed, and the pancreas was ablated directly through the surface of the pancreas with an HIFU transducer. In the Group B and Group C, extracorporeal HIFU ablation the pancreas was performed through intact skin. Animals in Group A and B were sacrificed immediately after HIFU procedures, whereas those in Group C at day 7 after HIFU. Experiments and animal care were carried out in compliance with the guide for the care and use of laboratory animals from the Ministry of Science and Technology of the People's Republic of China.
Instruments
HIFU ablation was performed with a HIFU tumor therapy system (Model JC type, Chongqing HaifuTech Co., Ltd, Chongqing City, China). The instrument was composed of three parts: a firing system located in a degassed water tank, an imaging system consisting of an ultrasound scanner coupled with a sterotaxic localizing arm, and a computer-controlled system for the firing sequence and the movement of the firing head in three dimensions.
Focused ultrasound was produced with a 12-cm diameter piezoelectric ceramic transducer. The system was operated using one of the several therapeutic transducers with the focal length of 90 to 160 mm. For each focal length, there is a choice of two transducers depending on the target depth: one operates at 0.8 MHz with 135-mm focal length and the other operates at 1.6 MHz with 90-mm focal length. The choice of transducers depends on the depth of target lesion, with the most commonly used parameters in this study were 0.8-MHz operating frequency and 135-mm focal length. In the centre of the transducer, there is a 3.5- to 5.0-MHz diagnostic ultrasound (US) imaging probe which is used as the real-time imaging unit of the system, guiding the target tissue volume, monitoring the energy deposition and the therapeutic effect, and also controlling the US exposure based on the feedback digital data from the ultrasonograms in the process of HIFU treatment. The therapeutic transducer and diagnostic imaging device were integrated into one transducer, and their beams were completely overlaid each other in the longitudinal diretion. The integrated transducer is moved by electric motors and can be moved smoothly in six directions, including three orthogonal directions (x, y, z), rotation along the ultrasound beam axis (θ), and rotation along the long or short axis of the bed (γ, φ) . Through computer control, the imaging probe was placed either against the skin or at a distance from the skin in water for pre-treatment imaging. The integrated transducer was mounted in a degassed water reservoir with the ultrasound beam directed upward. The ultrasound beam of the therapeutic transducer and the imaging probe overlapped completely, so that the longitudinal axis of the high-intensity focused ultrasound beam is in the two-dimensional US imaging plane. A calibrated polyvinylidene difluoride membrane hydrophone with a spot diameter of 0.5 mm was used to map the acoustic pressure field of the focused transducer at focal peak intensities of 200~300 W/cm2 [2]. The focal region was cigar shaped, with dimensions of 9.8 mm along the beam axis and 1.3 mm in the transverse direction. The absorbing target method was used to measure the total acoustic power output in degassed water at 21°C [6, 14].
HIFU procedure
The pigs were fasted for 72 h and then administered folium sennae tea to clean the intestinal tract. The skin covering the HIFU target area was shaved, washed with degassed water, and defatted with 75% alcohol solution before the procedure. Catheters were inserted into ear veins and ketamine was infused (50 mg/h) for anesthesia. Diazepam was administered as needed.
The HIFU ablation procedure complies with the guidance of the National Standard of China and was described in detail previously [6, 15, 16, 17]. In Group A, a laparotomy was performed and the pancreas was exposed followed by direct ablation of the head of the pancreas with a HIFU transducer. In Group B and C, the animals were fixed in a prone position. A rubber bag filled with degassed water was mounted between integrated transducer and the skin in order to well locate the target region. The real-time US imaging device was used to locate the head of pancreas as the pre-designed target region. The spatial volumes of the target regions in the X, Y and Z axes were 10×10×10 mm. There were three slices in the Z axes, so the interval distance between adjacent slices was 5 mm. The monitoring system of the therapeutic transducer was switched on for ablation (power, 220 W; frequency, 1.6MHz [Group A] and 0.8 MHz [Group B and C]; focal length, 90 mm [Group A] and 135 mm [Group B and C]). A focused US beam was mechanically scanned continuously at a speed of 0.5 to 3 mm/s. The treatment focus was moved from points to lines, then to planes and thereafter volume (total time of ablation: 145 s). Eventually the entire target region was covered by HIFU, leading the coagulation necrosis of the whole target regions. During the therapeutic process, real-time estimation of the therapeutic effect was carried out by the computer system through the graphic changes in the target field and the hyperecho of the tissues. Blood pressure, pulse, respiration, and blood oxygen saturation were monitored during HIFU treatment.
Animal care
The animals in Group A and B were sacrificed immediately after HIFU, and the whole pancreas was removed for histological examination. After HIFU treatment, the animals in Group C were fasted for 1 to 4 days until blood and urine amylase levels reached a normal level when these pig intravenously received penicillin (4.8×106 units), gentamycin (1.6×105 units), and ranitidine (100g) in 5% glucose saline (1500 ml) plus 10% glucose solution (1000 ml) daily. Then, they were allowed free access to a standard liquid diet. Vital signs and ultrasound-induced skin burns were monitored. Blood and urine samples were collected and leukocyte numbers, and levels of blood amylase, glucose, aspartate aminotransferase (AST), urea nitrogen (BUN) and total bilirubin were determined by Automatic Biochemical Analyzer (VITROS 250, Ortho-clinical diagnostics, Inc., NJ, USA) before the HIFU procedure and at days 1, 2, 3, 5 and 7 post-HIFU procedure. At day 7, the animals were sacrificed, and the whole pancreas was removed for histological examination.
Histological examination
The pancreas was stained with 1% 2,3,5-triphenyltetrazolium chloride (TTC) solution for 5 to 7 min, and then washed with water. Gross observations including the appearance, size and shape of pancreas were recorded. The necrosis volume was calculated as follow: 4/3π(A/2)×(B/2)×(C/2), where A, B, and C represent the three perpendicularly orientated diameters of the tumor. Then, the pancreas samples were fixed in 40 g/L formaldehyde salution, embedded in paraffin and stained with hematoxylin and eosin (H&E) for light microscopy (Olympus BH2, Olympus Corporation, Tokyo, Japan). Part of samples were processed for and evaluated by transmission electron microscopy (JEM-100CX, JEOL Ltd. Tokyo, Japan).
Statistical analysis
Data were expressed as means ± standard deviation (SD), and comparisons were performed with Wilcoxon rank sum test. All statistical analyses were carried out using SPSS software 12.5 for Windows (SPSS Inc., Chicago, IL, USA).
RESULTS
Survival of animals
Vital signs including blood pleasure, pulse, respiration, and blood oxygen saturation of all animals were stable during and after HIFU, demonstrating the pigs tolerated HIFU therapy. The animals in Group C recovered smoothly after HIFU treatment and survived for at least 7 days. Transient fatigue occurred and lasted for 1 to 3 days; however, no severe complications such as acute pancreatitis were observed. Mild skin burns at the HIFU sites were noted in two pigs in Group B and C.
Pathological presentations
After HIFU therapy, pale coagulation necrosis was easily identified in pancreas samples of all groups. Normal pancreatic tissues were red, whereas tissues of coagulation necrosis were white after TTC staining. In Group A and B, there was a sharp boundary between the HIFU necrosis and viable tissue (Fig. 1). In Group C, the treated tissues were shrunk and had clear boundaries at day 7 post-HIFU procedure. The irregularly-shaped necrotic regions were all smaller than 1 cm3, a theoretical necrosis volume. No significant difference in the necrotic tissue volume was observed among the three groups (Table 1), and thermolesions to intervening tissue were never observed.
HIFU therapeutic parameters
| Power (W) | Time (sec) | Necrosis volume (mm3) | Distance between skin and ablate foci (mm) | |
|---|---|---|---|---|
| Group A | 220 | 145 | 212.5 ± 25.3 | |
| Group B | 220 | 145 | 189.0 ± 39.8* | 47.2 ± 2.8△ |
| Group C | 220 | 145 | 198.0 ± 25.5* | 47.5±2.9△ |
W, watt. Data are expressed as mean ± SD; *P > 0.05; △P > 0.05.
TTC staining of pancreas at day 7 after HIFU. Coagulation necrosis (black arrow) was obvious and white arrow showed the normal pancreas. The boundary was clear.

Biochemistry results pre- and post-HIFU in group C
| Pre-HIFU | Day 0 | Day 1 | Day 2 | Day 3 | Day 5 | Day 7 | |
|---|---|---|---|---|---|---|---|
| Urine | |||||||
| Amylas (U/L) | 80.3±26.1 | 78.4±20.1 | 134.8±33.5 | 127.5±26.7 | 111.5±16.6 | 106.5±16.8 | 92.8±20.6 |
| Blood | |||||||
| Amylas (U/L) | 564.6±115.9 | 539.1±157.8 | 759.5±127.6 | 780.5±76.4 | 667.5±137.2 | 542.5±173.5 | 587.5±148.4 |
| Glucose (mmol/L) | 4.29±1.43 | 4.76±1.11 | 4.48±1.09 | 4.40±0.65 | 4.63±1.47 | 4.95±1.57 | 4.68 ±1.54 |
| Total bilirubin (μmol/L) | 14.4±6.1 | 15.3 ±6.3 | 16.9±4.9 | 19.9±4.4 | 12.1±3.1 | 12.2±3.2 | 11.2±2.5 |
| Leukocyte (×109/L) | 12.9±1.96 | 13.5±1.56 | 13.1±1.35 | 13.4±1.74 | 12.1±1.63 | 12.5±1.57 | 14.0±1.48 |
| AST (mmol/L) | 71.5±29.9 | 76.9±32.2± | 78.3±21.3 | 59.5±27.3 | 54.2±31.1 | 99.0±35.5 | 49.8±38.4 |
| BUN (mmol/L) | 3.24±0.89 | 3.99±1.71 | 4.30±1.60 | 3.09±2.19 | 4.25±1.09 | 3.42±1.21 | 3.60±0.80 |
Data are presented as means±SD; All dataP > 0.05 vs pre-HIFU.
AST:glutamic oxaloacetic transaminase; BUN: blood urea nitrogen.
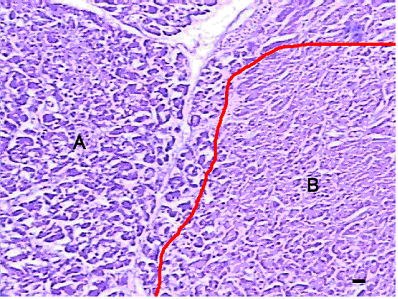
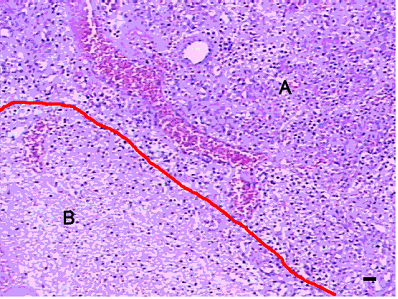
Under light microscope, the following characteristics of necrotic regions in the pancreas of Group A and B were present: karyopycnosis and nuclear fragmentation were observed in most of cells, and a sharp boundary between the normal tissue and target zones. Vascular proliferation and inflammatory hyperplasia were not evident (Fig. 2). Pancreatic samples in Group C at day 7 post-HIFU exhibited different features from those in Group A and B: target tissues were destroyed with necrotic cells and nuclear debris was observed in the necrotic regions. The pancreatic cells were amorphous, irregular, and bulky. A narrow region with inflammatory cell infiltration, consisting primarily of lymphocytes and monocytes sometimes with small number of eosinocytes, were seen between the necrotic and normal zones. In addition, hyperplasia of fibroblasts and collagen fibers were also noted in some regions (Fig. 3).
Presentations of pancreas in Group A and B under light microscope after HIFU (H&E, ×200). A apparent boundary was seen between normal (A) and target (B) tissues (red line). Scale bar =20 μm.
Presentations of pancreas in Group C under light microscope (H&E ×200), at day 7 after HIFU ablation. Infiltration of inflammatory cells and collagen fibers were observed and evident boundary between normal (A) and target (B) tissue was noted. Scale bar =20 μm.
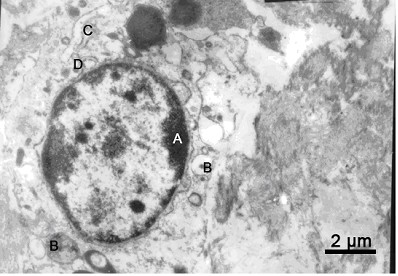
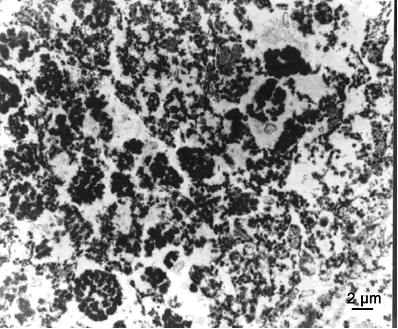
Under a transmission electron microscope, the following characteristics were observed in the necrotic regions of the Group A and Group B: the nuclear membrane had collapsed and chromatin was localized along the nuclear margin. Endochylema was vacuolated, and mitochondria swelled to a circular shape with a clear matrix and short or disappeared cristae, which were vacuolar appearances. Smooth and rough endoplasmic reticulum expanded and became vacuolar or fragmented (Fig. 4). At 7 day post-HIFU, in Group C, the cell membrane was completely destroyed and collapsed. The ultrastructures could not be identified, and apoptotic bodies were observed (Fig. 5).
Presentations of pancreas in Group A and B under transmission electron microscope (×10000). Chromatin margination (A), endochylema vacuolation (B), smooth endoplasmic reticulum expansion (C) and widened nuclear envelope (D) were observed.
Presentations of pancreas in Group C under transmission electron microscope (×10000) at day 7 after HIFU. The cell membrane was completely destroyed, and ultrastructures could not be identified.
Biochemistry parameters
In the present study, the amylase levels in the serum and urine were increased in the first 3 days and the first 5 days after HIFU ablation, respectively. But no significant difference was observed. Furthermore, the amylase levels were not 3 times higher than that before HIFU ablation. Moreover, there were not marked differences in the levels of other serum parameters between before and after HIFU ablation.
DISCUSSION
The ideal treatment of a localized cancer should achieve complete tumor cell death without damage to the adjacent tissues. HIFU is a minimally invasive technique that may induce complete coagulation necrosis of target tissues through intact skin. HIFU may be precisely focused on a tumour in the body. The acoustic energy passes through the intervening tissues to a tightly focused target region. The high powered focused beams employed are generated from sources placed either outside the body (for treatment of tumors of the liver, kidney, breast, uterus, pancreas and bone) or in the rectum (for treatment of the prostate), and are designed to enable rapid heating of a target tissue volume, while leaving tissue in the ultrasound propagation path relatively unaffected [18]. The mechanisms of HIFU ablation are primarily coagulation necrosis, acoustic cavitation, and apoptosis induced by hyperthermia [7, 19, 20, 21]. The rapid rate of energy deposition generates a rapid temperature increase (65oC-100oC), which results in irreversible cell death, with surrounding areas remaining largely unheated. In addition, HIFU can also activate the immune response [22, 23]. The minimal invasiveness and accurate targeting with a real-time US guide allow HIFU to precisely ablate lesions of large size, irregular shape, and even multi-modularity. A major advantage of HIFU over other thermal ablation techniques is that there is no necessity for the transcutaneous insertion of probes into the target tissue, which is not achievable with other conventional ablation techniques including percutaneous ethanol injection (PEI), radiofrequency (RF), interstitial laser coagulation (ILC), and cryotherapy [7, 20, 21]. Because HIFU is minimally invasive and accurate, and possesses real-time targeting, it provides patients with a new therapeutic option with less pain and damage to the splanchnic functions and fast recovery.
The pancreas, a deep abdominal organ surrounded by complicated anatomic structures, has an exocrine function and is sensitive to hyperthermia, which can result in the rupture of the pancreatic ducts and the surface membrane. The pancreatic enzymes can digest the pancreas itself, causing severe complications such as traumatic pancreatitis or pancreatogenic peritonitis. Thus, safety remains the main concern of any medical intervention of the pancreatic diseases.
A previous preclinical in vivo study in swine demonstrated the feasibility and safety of HIFU for pancreas ablation; however, histological assessment was performed only by light microscopy [13]. To our knowledge, in the present study, we for the first time used both light microscopy and transmission electron microscopy to determine the effects of HIFU on the pancreas. The histological presentations under light and transmission electron microscopes confirmed the efficacy and safety of HIFU by revealing complete necrosis only within the target regions and with clear boundary; the adjacent tissues were normal. Coagulation necrosis is characterized by dehydration and protein coagulation while the structural outline is still preserved for a long time. The mechanism of coagulation necrosis is still unclear. Lysosomal enzymes play no role in the process of coagulation necrosis, because the tissues have a small amount of lysosomes, or the lysosomal enzymes are also damaged under this circumstance. Acute pancreatitis is characterized by liquefaction necrosis, and lysosomal enzymes play an important role in the development and progression of pancreatitis. In present study, transmission electron microscopy was performed to observe the cell membrane and ultrastructures of cells. Results confirmed that, after HIFU ablation, coagulation necrosis occurred in the pancreas, and cell membrane, lysosomes and other organelles were intact. Therefore, a variety of digestive enzymes will not be released from cells, avoiding the liquefaction necrosis and subsequent pancreatitis. In addition, the rapid temperature increase by HIFU in pancreas deactivates pancreatic enzymes, and then prevents pancreatitis [24, 25]. In our study, light microscopy displayed abundant vacuoles of various sizes in the cytoplasm and chromatin margins and karyopyknosis in some cells. Electron microscopic examination revealed further details such as presence of karyopyknosis and chromatin margination in some cells, intercellular space widening, apoptotic bodies with high electron-density and numerous vacuoles of different sizes confirming the cavitation of HIFU.
During HIFU, vital signs of all pigs were stable. After HIFU, these animals returned to normal diet and recovered rapidly. In the present study, the amylase levels in the serum and urine were increased in the first 3 days and the first 5 days after HIFU ablation, respectively. But no significant difference was observed. Furthermore, the amylase levels were not 3 times higher than that before HIFU ablation, which was consistent with what Goldberg et al., reported [26]. Therefore, HIFU appears to be suitable for ablation of pancreatic tumors.
Pancreatic cancer is a type of tumors with poor blood supply. Blood vessels in the pancreatic tumors are thin without branches, which helps thermotherapies achieve good efficacy due to limited thermal diffusion [2]. HIFU is also able to collapse blood vessels smaller than 2 mm in diameter and block blood flow to the tumors [27]. Our results were consistent with the findings of Hwang et al [13].
Acoustic energy decreases gradually as it propagates through the intervening tissues. Anatomically the pancreas lies in deep abdomen and is surrounded by many important anatomic structures. The gas-containing organs such as the gastrointestinal (GI) tracts are poor transmitters of US beam which affects HIFU targeting and ablation [13]. In our pilot study, damage to the adjacent tissues was observed due to gas in the GI tracts. In the present study, we chose small mongrel pigs weighing only about 25 kg and carefully emptied the GI tract by fasting and senna-induced catharsis before HIFU. In addition, a rubber bag filled with degassed water was placed between the integrated transducer and skin. In Group B and C, a water bag with proper pressure was able to expel the intervening tissues and shorten the distance between the transducer and the pancreas. The necrotic volumes in Group A were somewhat larger than those in Group B and C (but not significant), probably due to the presence of gas ex vivo. In this study, the volumes of coagulation necrosis in all samples were within an ideal range. The actual biological focal regions might not be necessarily equal to physical focus regions in HIFU treatment [14].
In the present study, we demonstrated that HIFU is effective and safe for the ablation of the pancreas in a swine model. Our results provide evidence supporting the clinical application of HIFU in patients with pancreatic cancer.
Conflict of Interest
The authors have declared that no conflict of interest exists.
References
1. Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, Thun MJ. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71-96
2. Sarkar FH, Banerjee S, Li Y. Pancreatic cancer: pathogenesis, prevention and treatment. Toxicol Appl Pharmacol. 2007;224:326-36
3. Lynn JG, Zwemer RL, Chick AJ, Miller AE. A new method for the ceneration and use of focused ultrasound in experimental biology. J Gen Physiol. 1942Nov20;26(2):179-193
4. Burov AK. High-intensity ultrasonic vibrations for action on animal and human malignant tumors. Dokl Akad Nauk SSSR. 1956;106:239-41
5. Wu F. Extracorporeal high intensity focused ultrasound in the treatment of patients with solid malignancy. Minim Invasive Ther Allied Technol. 2006;15:26-35
6. Li YY, Sha WH, Zhou YJ, Nie YQ. Short and long term efficacy of high intensity focused ultrasound therapy for advanced hepatocellular carcinoma. J Gastroenterol Hepatol. 2007;22:2148-54
7. Dubinsky TJ, Cuevas C, Dighe MK, Kolokythas O, Hwang JH. High-intensity focused ultrasound: current potential and oncologic applications. AJR Am J Roentgenol. 2008;190:191-9
8. Wu F, Wang ZB, Chen WZ, Wang W, Gui Y, Zhang M, Zheng G, Zhou Y, Xu G, Li M, Zhang C, Ye H, Feng R. Extracorporeal high intensity focused ultrasound ablation in the treatment of 1038 patients with solid carcinomas in China: an overview. Ultrason Sonochem. 2004;11:149-54
9. Leslie TA, Kennedy JE. High intensity focused ultrasound in the treatment of abdominal and gynaecological diseases. Int J Hyperthermia. 2007;23:173-82
10. Jolesz FA, Hynynen K, McDannold N, Freundlich D, Kopelman D. Noninvasive thermal ablation of hepatocellular carcinoma by using magnetic resonance imaging-guided focused ultrasound. Gastroenterology. 2004;127:S242-7
11. Wang X, Sun J. High-intensity focused ultrasound in patients with late-stage pancreatic carcinoma. Chin Med J (Engl). 2002;115:1332-5
12. Wu F, Wang ZB, Zhu H, Chen WZ, Zou JZ, Bai J, Li KQ, Jin CB, Xie FL, Su HB. Feasibility of US-guided high-intensity focused ultrasound treatment in patients with advanced pancreatic cancer: initial experience. Radiology. 2005;236:1034-40
13. Hwang JH, Wang YN, Warren C, Upton MP, Starr F, Zhou Y, Mitchell SB. Preclinical in vivo evaluation of an extracorporeal HIFU device for ablation of pancreatic tumors. Ultrasound Med Biol. 2009;35:967-75
14. Wang Z, Bai J, Li F, Du Y, Wen S, Hu K, Xu G, Ma P, Yin N, Chen W, Wu F, Feng R. Study of a “biologic focal region” of high-intensity focused ultrasound. Ultrasound Med Biol. 2003;29:749-754
15. ter Haar GR, Kennedy JE, Wu F. Physical characterization of extracorporeal high intensity focused ultrasound (HIFU) treatments of cancer. Ultrasound Med Biol. 2004 in press
16. Wu F, Chen WZ, Bai J, Zou JZ, Wang ZL, Zhu H, Wang ZB. Pathological changes in human malignant carcinoma treated with high-intensity focused ultrasound. Ultrasound Med Biol. 2001Aug;27(8):1099-106
17. Ministry of Health of the P.R.C. Guideline for the clinical application of high intensity focused ultrasound in malignancies (advance copy). Natl Med J China. 2005;85(12):796-797
18. Haar GT, Coussios C. High intensity focused ultrasound: physical principles and devices. Int J Hyperthermia. 2007;23:89-104
19. ter Haar G. Therapeutic applications of ultrasound. Prog Biophys Mol Biol. 2007;93:111-29
20. Kennedy JE, Ter Haar GR, Cranston D. High intensity focused ultrasound: surgery of the future? Br J Radiol. 2003;76:590-9
21. Hill CR, ter Haar GR. Review article: high intensity focused ultrasound--potential for cancer treatment. Br J Radiol. 1995;68:1296-1303
22. Wu F, Wang ZB, Lu P, Xu ZL, Chen WZ, Zhu H, Jin CB. Activated anti-tumor immunity in cancer patients after high intensity focused ultrasound ablation. Ultrasound Med Biol. 2004;30:1217-22
23. Miller DL, Song J. Tumor growth reduction and DNA transfer by cavitation-enhanced high-intensity focused ultrasound in vivo. Ultrasound Med Biol. 2003;29:887-93
24. Clarke RL, ter Haar GR. Temperature rise recorded during lesion formation by high-intensity focused ultrasound. Ultrasound Med Biol. 1997;23:299-306
25. Macdonald NJ, Jolesz FA, Hynynen KH. Determination of the optimal delay between sonications during focused ultrasound surgery in rabbit by using MR imaging to monitor thermal build up in vivo. Radiology. 1999;211:419-426
26. Goldberg SN, Mallery S, Gazelle GS, Brugge WR. EUS-guided radiofrequency ablation in the pancreas: results in a porcine model. Gastrointest Endosc. 1999;50:392-401
27. Vaezy S, Zderic V. Hemorrhage control using high intensity focused ultrasound. Int J Hyperthermia. 2007;23(2):203-11
Author contact
![]() Corresponding author: Professor Lin Jia, Department of Gastroenterology, Guangzhou First Municipal People's Hospital, Guangzhou Nan Sha Center Hospital Affiliated to Guangzhou Medical College, Guangzhou, Guangdong Province 510180, China. E-mail: fastmotionnet; Tel: +8620 81628809; Fax: +8620 81628809.
Corresponding author: Professor Lin Jia, Department of Gastroenterology, Guangzhou First Municipal People's Hospital, Guangzhou Nan Sha Center Hospital Affiliated to Guangzhou Medical College, Guangzhou, Guangdong Province 510180, China. E-mail: fastmotionnet; Tel: +8620 81628809; Fax: +8620 81628809.