International Journal of Medical Sciences
ISSN: 1449-1907
3.2
Impact Factor
ISSN: 1449-1907

 Global reach, higher impact
Global reach, higher impactInt J Med Sci 2010; 7(1):48-54. doi:10.7150/ijms.7.48 This issue Cite
Research Paper
Effect of dose-escalation of 5-fluorouracil on circadian variability of its pharmacokinetics in Japanese patients with Stage III/IVa esophageal squamous cell carcinoma
Akiko Kuwahara1, Motohiro Yamamori2, Kohshi Nishiguchi 3,4, Tatsuya Okuno 3, Naoko Chayahara 3, Ikuya Miki 3, Takao Tamura 3, Kaori Kadoyama2, Tsubasa Inokuma 2, Yoshiji Takemoto 2, Tsutomu Nakamura3, Kazusaburo Kataoka 1, Toshiyuki Sakaeda 2,3 ![]()
1. School of Pharmacy and Pharmaceutical Sciences, Mukogawa Women's University, Nishinomiya 663-8179, Japan
2. Graduate School of Pharmaceutical Sciences, Kyoto University, Kyoto 606-8501, Japan
3. Kobe University Graduate School of Medicine, Kobe 650-0017, Japan
4. Faculty of Pharmaceutical Sciences, Kyoto Pharmaceutical University, Kyoto 607-8414, Japan
Received 2009-10-14; Accepted 2010-1-28; Published 2010-1-31
Citation:
Kuwahara A, Yamamori M, Nishiguchi K, Okuno T, Chayahara N, Miki I, Tamura T, Kadoyama K, Inokuma T, Takemoto Y, Nakamura T, Kataoka K, Sakaeda T. Effect of dose-escalation of 5-fluorouracil on circadian variability of its pharmacokinetics in Japanese patients with Stage III/IVa esophageal squamous cell carcinoma. Int J Med Sci 2010; 7(1):48-54. doi:10.7150/ijms.7.48. https://www.medsci.org/v07p0048.htm
Other stylesAbstract
Objective: The effects of dose-escalation of 5-fluorouracil (5-FU) on the clinical outcome and pharmacokinetics of 5-FU were investigated in Japanese patients with Stage III/IVa esophageal squamous cell carcinoma.
Methods: Thirty-five patients with Stage III/IVa were enrolled, who were treated with a definitive 5-FU/cisplatin-based chemoradiotherapy. A course consisted of continuous infusion of 5-FU at 400 mg/m2/day (the standard dose group, N=27) or 500-550 mg/m2/day (the high dose group, N=8) for days 1-5 and 8-12, infusion of cisplatin at 40 mg/m2/day on days 1 and 8, and radiation at 2 Gy/day on days 1 to 5, 8 to 12, and 15 to 19, with a second course repeated after a 2-week interval. Plasma concentrations of 5-FU were determined by high performance liquid chromatography at 5:00 PM on days 3, 10, 38 and 45, and at 5:00 AM on days 4, 11, 39 and 46.
Results and conclusions: No patient with Stage IVa achieved a complete response in the standard dose group, whereas a complete response was observed at a rate of 50% in the high dose group, and this can be explained by a higher plasma concentration of 5-FU. The circadian rhythm in the concentrations found at the standard dose was not observed for a higher dose.
Keywords: esophageal squamous cell carcinoma, 5-fluorouracil, plasma concentration, circadian rhythm, dose-escalation
Introduction
A clinical report published in 1999, the RTOG (Radiation Therapy Oncology Group) 85-01 trial involving 134 patients with T1-3, N0-1 and M0 esophageal cancer, is of great interest in terms of clinical outcome because it demonstrated a 5-year survival rate of 26 % [1-4]. This treatment consists of a 96-hr-infusion of 5-fluorouracil (5-FU) at a daily dose of 1,000 mg/m2/day in weeks 1, 5, 8 and 11, infusion of cisplatin (CDDP) at 75 mg/m2/day on the first day of week 1, 5, 8 and 11, and concurrent radiation at 50 Gy in 25 fractions over 5 weeks, without pre- or post-surgical resection. The total dose of 5-FU and CDDP was 16,000 mg/m2 and 300 mg/m2, respectively.
Simultaneously in Japan, a dose-reduction version was proposed by Ohtsu and his co-workers for advanced metastatic esophageal squamous cell carcinoma (ESCC) which consists of a 120-hr-infusion of 5-FU at 400 mg/m2/day in weeks 1, 2, 6 and 7, infusion of CDDP at 40 mg/m2/day on the first day of week 1, 2, 6 and 7, and concurrent radiation at 60 Gy in 30 fractions over 8 weeks [5,6]. The total dose of 5-FU and CDDP was 8,000 mg/m2 and 160 mg/m2, respectively, being about half of those in the RTOG 85-01. Two independent clinical investigations have shown curative potential using this regimen for unresectable ESCC with T4 or M1a [5,6]. A long-term evaluation of efficacy and toxicity with 139 patients resulted in a complete response (CR) rate of 56%, along with a 5-year survival rate of 29 % [7-9]. Currently, a definitive 5-FU/CDDP-based chemoradiotherapy (CRT) is recognized as one of the most promising treatments for esophageal cancer [10], and future improvements will likely require the modification of the RTOG 85-01 regimen or Ohtsu's regimen, and incorporation of a novel anticancer drug.
A series of studies has been performed to find a marker predictive of clinical outcome after treatment with the Ohtsu's regimen [11-13]. A total of 8 measurements of the plasma concentration of 5-FU were made per patient, and it was concluded that the average value was predictive of clinical response, but not of severe acute leucopenia, stomatitis and cheilitis [13]. The average concentration in the patients with CR was 0.122±0.035 μg/mL, and was significantly higher than that in non-CR patients, 0.102±0.023 μg/mL (p = 0.029) [13]. A CR was not observed in 7 patients with Stage IVa, but the concentration tended to be lower in such patients, 0.102±0.028 μg/mL [13], suggesting that the dose- escalation of 5-FU results in a CR even in the patients with Stage IVa.
Although little information is available for dose-escalation of 5-FU, CDDP or radiation in advanced esophageal cancer, Yamashita et al. have applied the RTOG 85-01 protocol [14-17], and two Phase II trials, referred to as JCOG (Japan Clinical Oncology Group Trial) 9516 and 9407, have been performed for advanced ESCC in Japan [18,19]. In this study, based on the Ohtsu's regimen, a dose-escalation of 5-FU from 400 mg/m2/day to 500-550 mg/m2/day was applied to ESCC patients with Stage III/IVa, and the preliminary results are summarized with regard to clinical outcome and plasma concentrations of 5-FU.
Patients and Methods
Patients
Thirty-five ESCC patients were enrolled in this study, 27 of whom were treated with 400 mg/m2/day of 5-FU (the standard dose group), and the remaining 8 of whom were treated at 500-550 mg/m2/day (the high dose group). The patients were recruited based on the following criteria: 1) ESCC treated at Kobe University Hospital from August 2002 to June 2006; 2) Stage III (T3/T4, N1, M0) or IVa (T1-T4, N0/N1, M1a) according to the International Union Against Cancer tumor node metastasis (TNM) classification; 3) age less than 85 years; 4) an Eastern Cooperative Oncology Group performance status of 0 to 2; 5) adequate bone marrow, renal, and hepatic function; 6) no prior chemotherapy; 7) no severe medical complications; and 8) no other active malignancies (except early cancer). The tumors were histologically confirmed to be primary.
Protocol
The protocol is presented in Figure 1. A course consisted of continuous infusion of 5-FU at 400 or 500-550 mg/m2/day for days 1-5 and 8-12, infusion of CDDP at 40 mg/m2/day on days 1 and 8, and radiation at 2 Gy/day on days 1 to 5, 8 to 12, and 15 to 19, with a second course repeated after a 2-week interval [5,6]. If disease progression/recurrence was observed, either salvage surgery, endoscopic treatment, or another regimen of chemotherapy was scheduled. This study was conducted with the authorization of the institutional review board and followed the medical research council guidelines of Kobe University.
Determination of Plasma Concentration of 5-FU
Aliquots (5 mL) of blood were collected into etylenediaminetetraacetic acid-treated tubes at 5:00 PM on days 3, 10, 38 and 45, and at 5:00 AM on days 4, 11, 39 and 46 [11-13]. The plasma concentrations of 5-FU were determined by high-performance liquid chromatography as described previously [11-13].
Clinical Response
The clinical response was evaluated according to the method reported previously [5-9]. Briefly, a CR was defined as the complete disappearance of all measurable and assessable disease at the first evaluation, which was performed 1 month after the completion of CRT to determine whether the disease had progressed. The clinical response was evaluated by endoscopy and chest and abdominal computed tomography (CT) scans in each course. A CR at the primary site was evaluated by endoscopic examination when all of the following criteria were satisfied on observation of the entire esophagus: 1) disappearance of the tumor lesion; 2) disappearance of ulceration (slough); and 3) absence of cancer cells in biopsy specimens. If small nodes of 1 cm or less were detected on CT scans, the recovery was defined as an “uncertain CR” after confirmation of no progression for at least 3 months. An “uncertain CR” was included as a CR when calculating the CR rate. When these criteria were not satisfied, a non-CR was assigned. The existence of erosion, a granular protruded lesion, an ulcer scar, and 1.2 w/v% iodine/glycerin-voiding lesions did not prevent an evaluation of CR. The evaluations were performed every month for the first 3 months, and when the criteria for CR were not satisfied at 3 months, the result was changed to non-CR. Follow-up evaluations were performed thereafter every 3 months for 3 years by endoscopy and CT scan. After 3 years, patients were seen every 6 months. During the follow-up period, a routine course of physical examinations and clinical laboratory tests was performed to check the patient's health.
Severe Acute Toxicities
A definitive 5-FU/CDDP-based CRT is associated with acute toxicities; leucopenia, anemia, thrombocytopenia, nausea/vomiting, diarrhea, mucositis (including stomatitis), esophagitis, and renal dysfunction [5-9, 20]. Here, severe acute leucopenia, stomatitis, and cheilitis were subjected into the analysis. Toxicity was evaluated using criteria defined by the Japan Clinical Oncology Group [21]. These criteria were based on the National Cancer Institute Common Toxicity Criteria. Toxicity was assessed on a 2 to 3 day basis during the CRT and subsequent hospitalization period and on every visit after the completion of CRT. Episodes of leucopenia, stomatitis, and cheilitis during the first 2 courses and subsequent 2 weeks (until day 70) were recorded as acute toxicities and those of grade 3 or more as severe acute toxicities.
Data Analysis and Statistics
All values reported are the mean±standard deviation (SD). Circadian variations of plasma concentrations of 5-FU were analyzed with the Wilcoxon signed-rank test. The unpaired Student's t-test/Welch's test or Mann-Whitney's U test was used for two-group comparisons of the concentrations. Fisher's exact test was used for the analysis of contingency tables. P values of less than 0.05 (two tailed) were considered to be significant.
Figure 1
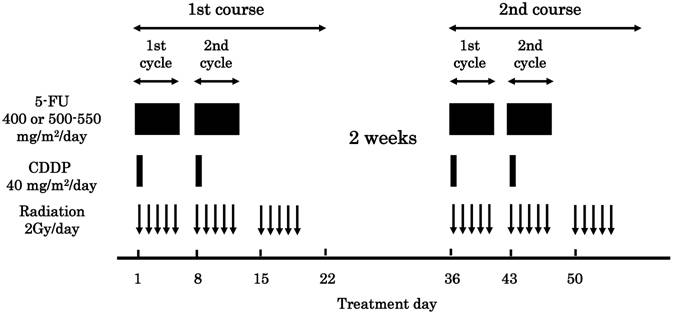
Protocol of a definitive 5fluorouracil (5-FU)/ cisplatin (CDDP)-based chemoradiotherapy. One course of treatment consisted of protracted venous infusions of 5-FU (400 or 500-550 mg/m2/day for days 1-5 and 8-12) and CDDP (40 mg/m2/day on days 1 and 8), and radiation (2 Gy/day on days 1-5, 8-12, and 15-19), with a second course (days 36-56) repeated after a 2-week interval.
Results
Demographic and clinicopathologic characteristics of the 35 Japanese ESCC patients are summarized in Table 1. There was no difference between the standard dose group and high dose group, concerning age, height, weight, sex, performance status, differentiation, TNM score and clinical stage. Table 2 shows the results of clinical outcome. The overall CR rate was 22.2 % and 37.5 % for the standard dose group and high dose group, respectively. In the standard dose group, all 6 CR patients were at Stage III, and none of Stage IVa patients had a CR. In contrast, 2 of 4 Stage IVa patients had a CR in the high dose group. Severe acute leucopenia, stomatitis or cheilitis were found at a rate of 37.0%, 14.8% and 18.5%, respectively, and nausea/vomiting and diarrhea were found in a few patients (ca. 10%). There was no significant increase in the rate of severe acute toxicities, according to the increase in the dose of 5-FU.
The values of the plasma concentrations of 5-FU are listed in Table 3. The average of 8 measurements made per patient is listed as the data. The plasma concentrations of 5-FU in the high dose group, 0.137±0.031 μg/mL, were higher than those in the standard dose group, 0.112±0.030 μg/mL, but with no statistical significance (p = 0.052), presumably due to great differences between individuals. In Stage IVa, the plasma concentrations of 5-FU in the high dose group, 0.144±0.029 μg/mL, were significantly higher than those in the standard dose group, 0.101±0.027 μg/mL (p = 0.028), and tended to be still higher after the dose-normalization (0.116±0.012 μg/mL). The plasma concentration of 5-FU was 0.131 μg/mL and 0.182 μg/mL in 2 Stage IVa patients with a CR.
The circadian variation in the plasma concentration of 5-FU is shown in Figure 2 and the differences between the two groups are summarized in Table 4. In the standard dose group, the plasma concentrations of 5-FU at 5:00 AM (0.069±0.031 μg/mL) were significantly lower than those at 5:00 PM (0.109±0.059 μg/mL) in the 1st cycle/1st course (P < 0.05, β = 0.882) and a similar tendency was observed in the 2nd cycle/1st course (P = 0.438, β = 0.179), not significantly. The plasma concentrations of 5-FU at 5:00 PM and 5:00 AM in the second cycle were both significantly higher than those in the first cycle, and these phenomena found in the first course were also observed in the second course. As for the high dose group, the plasma concentrations of 5-FU at 5:00 AM (0.073±0.049 μg/mL) were significantly lower than at 5:00 PM (0.119±0.043 μg/mL) in the 1st cycle/1st course (P < 0.05, β = 0.902), but those at 5:00 AM were higher than those at 5:00 PM in the 2nd cycle/1st course (not significantly). The plasma concentrations of 5-FU at 5:00 PM and 5:00 AM in the second cycle were both higher than those in the first cycle. In the second course, the circadian variation found in the first course was not observed. As shown in Table 4, the concentrations in the high dose group were higher than those in the standard dose group, but the increase was relatively remarkable at 5:00 AM than 5:00 PM.
Table 1
Demographic and Clinicopathologic Characteristics of 35 Japanese Patients with Esophageal Squamous Cell Carcinoma
| Group | Standard dose a) | High dose | p d) |
|---|---|---|---|
| N | 27 | 8 | |
| Age, yr | 63.0±7.8 (48 -75) b) | 62.5±5.0 (56 -71) | 0.865 |
| Height, cm | 162.9±7.1 (150-180) | 164.2±4.6 (159-172) | 0.633 |
| Weight, kg | 55.2±9.3 (33-79) | 55.3±7.6 (46-72) | 0.919 |
| Male/Female | 24/3 | 8/0 | 1.000 |
| Performance status, 0/1/2/unknown | 11/13/2/1 | 4/4/0/0 | 1.000 |
| Differentiation, well/moderate/poor/unknown | 3/13/6/5 | 1/1/3/3 | 0.266 |
| T1/T2/T3/T4 | 1/1/13/12 | 0/0/6/2 | 0.655 |
| N0/N1 | 3/24 | 1/7 | 1.000 |
| M0/M1a c) | 19/8 | 4/4 | 0.402 |
| Stage III/IVa | 19/8 | 4/4 | 0.402 |
a) Standard dose group: 400 mg/m2/day of 5-fluorouracil; High dose group: 500-550 mg/m2/day of 5-fluorouracil.
b) The values are the mean±SD, with the range in parentheses.
c) Noncervical primary tumors with positive supraclavicular lymph nodes were defined as M1a.
d) Standard dose group vs. high dose group (see the section “PATIENTS AND METHODS”).
Table 2
Clinical Outcome in 35 Japanese Patients with Esophageal Squamous Cell Carcinoma
| Group | Standard dose a) | High dose | p c) | |
|---|---|---|---|---|
| N | 27 | 8 | ||
| Clinical Response | ||||
| Complete response (CR) rate b) | 6 (22.2 %) | 3 (37.5 %) | 0.396 | |
| Severe Acute Toxicity (Grade 3/4) | ||||
| Leucopenia | 10 (37.0 %) | 4 (50.0 %) | 0.685 | |
| Stomatitis | 4 (14.8 %) | 1 (12.5 %) | 1.000 | |
| Cheilitis | 5 (18.5 %) | 2 (25.0 %) | 0.648 | |
a) Standard dose group: 400 mg/m2/day of 5-fluorouracil; High dose group: 500-550 mg/m2/day of 5-fluorouracil.
b) Two of 4 patients with Stage IVa had a CR in the high dose group, but no patient in the standard dose group.
c) Standard dose group vs. high dose group (Fisher's exact test).
Table 3
Association of Disease Stage with Plasma Concentrations (μg/mL) of 5Fluorouracil in the Standard dose and High dose groups.
| Group | Standard dose a) | High dose | p c) | ||
|---|---|---|---|---|---|
| Stage III | 19 | 0.117±0.031 b) | 4 | 0.131±0.036 | 0.454 |
| Stage IVa | 8 | 0.101±0.027 | 4 | 0.144±0.029 | 0.028 |
| Stage III/ IVa | 27 | 0.112±0.030 | 8 | 0.137±0.031 | 0.052 |
a) Standard dose group: 400 mg/m2/day of 5-fluorouracil; High dose group: 500-550 mg/m2/day of 5-fluorouracil.
b) The values are the mean±SD. The average of 8 measurements made per patient is listed as the data.
c) Standard dose group vs. high dose group (see the section “PATIENTS AND METHODS”).
Table 4
Plasma Concentrations (μg/mL) of 5Fluorouracil in the Standard dose and High dose groups.
| Group | Standard dose a) | High dose | p c) | |
|---|---|---|---|---|
| N | 27 | 8 | ||
| 1st cycle / 1st course | ||||
| Day3 5:00 PM | 0.109±0.059 b) | 0.119±0.043 | 0.665 | |
| Day4 5:00 AM | 0.069±0.031 | 0.073±0.049 | 0.758 | |
| 2nd cycle / 1st course | ||||
| Day10 5:00 PM | 0.143±0.053 | 0.157±0.050 | 0.515 | |
| Day11 5:00 AM | 0.132±0.048 | 0.170±0.057 | 0.084 | |
| 1st cycle / 2nd course | ||||
| Day38 5:00 PM | 0.112±0.047 | 0.134±0.081 | 0.412 | |
| Day39 5:00 AM | 0.073±0.042 | 0.136±0.058 | 0.004 | |
| 2nd cycle / 2nd course | ||||
| Day45 5:00 PM | 0.148±0.090 | 0.158±0.074 | 0.509 | |
| Day46 5:00 AM | 0.115±0.038 | 0.172±0.090 | 0.151 | |
a) Standard dose group: 400 mg/m2/day of 5-fluorouracil; High dose group: 500-550 mg/m2/day of 5-fluorouracil.
b) The values are the mean±SD.
c) Standard dose group vs. high dose group (see the section “PATIENTS AND METHODS”).
Figure 2
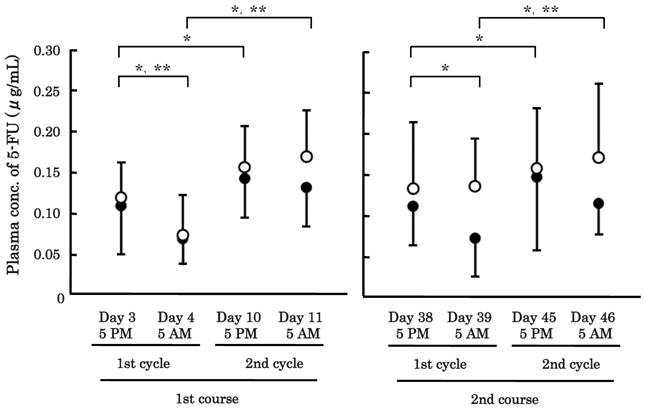
Circadian variation of plasma concentrations of 5fluorouracil (5-FU) in patients with advanced esophageal cancer. A total of 8 measurements were made per patient: 5:00 PM on days 3, 10, 38 and 45, and 5:00 AM on days 4, 11, 39 and 46. Closed circle: the standard dose group (N=27), open circle: the high dose group (N=8). The bars represent the SD. * P < 0.05 in the standard dose group, ** P < 0.05 in the high dose group.
Discussion
Esophageal cancer is the 8th most common cancer in the world and one of the most lethal [10]. Symptoms include dysphagia, odynophagia, and progressive weight loss. The two predominant histological subtypes are adenocarcinoma and squamous cell carcinoma, and treatment depends on the location of the primary tumor, the disease stage, patient characteristics and co-morbidities, and occasionally, histological subtype. There is no consensus on an optimal treatment strategy for esophageal cancer, and treatments include surgical procedures, radiation, chemotherapy, and combinations thereof [10]. In patients with localized squamous cell carcinoma, a definitive 5-FU/CDDP-based CRT is one of the most promising ways to achieve a complete pathologic response. The treatment might be improved further through modification of the treatment schedule, dose escalation and the replacement of 5-FU and CDDP.
Yamashita et al. have demonstrated that the RTOG 85-01 regimen is well tolerable for Japanese patients, where 44 patients with Stage I/II/III/IV = 9/9/15/11 were enrolled and the CR rate was 71 % [16]. In this study, a dose-escalation of 5-FU from 400 mg/m2/day to 500-550 mg/m2/day was applied to advanced ESCC patients with Stage III/IVa, based on Ohtsu's regimen. The dose was defined according to our clinical investigations, and it was found that this slight dose escalation is also acceptable for Japanese patients. The frequency of severe acute leucopenia increased a little. It has been demonstrated that the overall CR rate was improved slightly by increased amounts of 5-FU. No patient with Stage IVa achieved a CR in the standard dose of 5-FU, but 2 of 4 patients achieved a CR in the high dose group (Table 2). This can be explained by a higher plasma concentration of 5-FU in the patients (Table 3). It is noted that the concentrations were still higher after the dose-normalization, suggesting saturation of the elimination of 5-FU, especially in Stage IVa.
Here, it was confirmed that a circadian rhythm exists in the concentrations of 5-FU at the standard dose (Figure 2). The concentrations were lower in the morning than the evening. It is well-known that there is a circadian rhythm in drug metabolism, cellular proliferation and physiological function, and the suprachiasmatic nuclei, a hypothalamic pacemaker clock, is important for the rhythm [22-24]. As a result, both the toxicity and efficacy of over 30 anticancer agents vary as a function of dosing time [22-24]. More than 80 % of the administered 5-FU is eliminated by the rate-limiting enzyme, dihydropyrimidine dehydrogenase (DPD). The DPD activity is found in most tissues, but is highest in the liver. The activity of DPD of diurnally active cancer patients varies significantly during a 24-hour time period, and is greatest from midnight to early morning [23-26], being consistent with the findings of this study. In addition, it was found that the circadian rhythm observed in the patients treated with the standard dose is not recognized of the higher dose. The DPD activity is inhibited by 5-FU administration [22], and this might contribute to the increase in the concentration of 5-FU in the second cycle compared to the first cycle in the standard dose group, shown in Figure 2. The disappearance of circadian rhythm in the 5-FU plasma concentration of the higher dose can be explained by the inhibition of DPD.
In conclusion, the dose-escalation of 5-FU results in a preferable clinical response, especially in advanced ESCC patients, and this is explained, in part, by a higher plasma concentration of 5-FU. The circadian rhythm found with the standard dose is not observed for a higher dose. Chronotherapy of 5-FU is believed to be a promising way to optimize cancer chemotherapy, and further clinical investigation should be performed on the impact of dose-escalation, with a large number of patients.
Acknowledgements
This work was supported in part by a Grant-in-Aid for Scientific Research and Service Innovation Program from the Ministry of Education, Culture, Sports, Science and Technology of Japan.
Competing Interest
The authors declare that no conflict of interest exists.
References
1. Cooper JS, Guo MD, Herskovic A. et al. Chemoradiotherapy of locally advanced esophageal cancer: long-term follow-up of a prospective randomized trial (RTOG 85-01). Radiation Therapy Oncology Group. JAMA. 1999;281:1623-7
2. Herskovic A, Martz K, Al-Sarraf M. et al. Combined chemotherapy and radiotherapy compared with radiotherapy alone in patients with cancer of the esophagus. N Eng J Med. 1992;326:1593-8
3. Begg C, Cho M, Eastwood S. et al. Improving the quality of reporting of randomized controlled trials. The CONSORT statement. JAMA. 1996;276:637-9
4. Al-Sarraf M, Martz K, Herskovic A. et al. Progress report of combined chemoradiotherapy versus radiotherapy alone in patients with esophageal cancer: an intergroup study. J Clin Oncol. 1997;15:277-84
5. Ohtsu A, Boku N, Muro K. et al. Definitive chemoradiotherapy for T4 and/or M1 lymph node squamous cell carcinoma of the esophagus. J Clin Oncol. 1999;17:2915-21
6. Kaneko K, Ito H, Konishi K. et al. Definitive chemoradiotherapy for patients with malignant stricture due to T3 or T4 squamous cell carcinoma of the oesophagus. Br J Cancer. 2003;88:18-24
7. Tahara M, Ohtsu A, Hironaka S. et al. Clinical impact of criteria for complete response (CR) of primary site to treatment of esophageal cancer. Jpn J Clin Oncol. 2005;35:316-23
8. Ishikura S, Nihei K, Ohtsu A. et al. Long-term toxicity after definitive chemoradiotherapy for squamous cell carcinoma of the thoracic esophagus. J Clin Oncol. 2003;21:2697-702
9. Kumekawa Y, Kaneko K, Ito H. et al. Late toxicity in complete response cases after definitive chemoradiotherapy for esophageal squamous cell carcinoma. J Gastroenterol. 2006;41:425-32
10. Sakaeda T, Yamamori M, Kuwahara A. et al. Pharmacokinetics and pharmacogenomics in esophageal cancer chemoradiotherapy. Adv Drug Deliv Rev. 2009;61:388-401
11. Miki I, Tamura T, Nakamura T. et al. Circadian variability of pharmacokinetics of 5-fluorouracil and CLOCK T3111C genetic polymorphism in patients with esophageal carcinoma. Ther Drug Monit. 2005;27:369-74
12. Okuno T, Tamura T, Yamamori M. et al. Favorable genetic polymorphisms predictive of clinical outcome of chemoradiotherapy for Stage II/III esophageal squamous cell carcinoma in Japanese. Am J Clin Oncol. 2007;30:252-7
13. Sakaeda T, Yamamori M, Kuwahara A. et al. VEGF G-1154A is predictive of severe acute toxicities during chemoradiotherapy for esophageal squamous cell carcinoma in Japanese patients. Ther Drug Monit. 2008;30:497-503
14. Yamashita H, Nakagawa K, Tago M. et al. The experience of concurrent chemoradiation for Japanese patients with superficial esophageal squamous cell carcinoma: a retrospective study. Am J Clin Oncol. 2005;28:555-9
15. Yamashita H, Nakagawa K, Yamada K. et al. A single institutional non-randomized retrospective comparison between definitive chemoradiotherapy and radical surgery in 82 Japanese patients with resectable esophageal squamous cell carcinoma. Dis Esophagus. 2008;21:430-6
16. Yamashita H, Nakagawa K, Tago M. et al. The intergroup/RTOG 85-01 concurrent chemoradiation regimen for Japanese esophageal cancer. Hepatogastroenterology. 2006;53:863-8
17. Yamashita H, Nakagawa K, Tago M. et al. Treatment results of preoperative concurrent chemoradiotherapy followed by surgery for Stage III or IV esophageal squamous cell carcinoma. Radiat Med. 2006;24:65-71
18. Ishida K, Ando N, Yamamoto S. et al. Phase II study of cisplatin and 5-fluorouracil with concurrent radiotherapy in advanced squamous cell carcinoma of the esophagus: a Japan Esophageal Oncology Group (JEOG)/Japan Clinical Oncology Group trial (JCOG9516). Jpn J Clin Oncol. 2004;34:615-9
19. Hayashi K, Ando N, Watanabe H. et al. Phase II evaluation of protracted infusion of cisplatin and 5-fluorouracil in advanced squamous cell carcinoma of the esophagus: a Japan Esophageal Oncology Group (JEOG) Trial (JCOG9407). Jpn J Clin Oncol. 2001;31:419-23
20. Hironaka S, Ohtsu A, Boku N. et al. Nonrandomized comparison between definitive chemoradiotherapy and radical surgery in patients with T(2-3)N(any) M(0) squamous cell carcinoma of the esophagus. Int J Radiat Oncol Biol Phys. 2003;57:425-33
21. Tobinai K, Kohno A, Shimada Y. et al. Toxicity grading criteria of the Japan Clinical Oncology Group (The Clinical Trial Review Committee of the Japan Clinical Oncology Group). Jpn J Clin Oncol. 1993;23:250-7
22. Milano G, Chamorey AL. Clinical pharmacokinetics of 5-fluorouracil with consideration of chronopharmacokinetics. Chronobiol Int. 2002;19:177-89
23. Lévi F, Focan C, Karaboué A. et al. Implications of circadian clocks for the rhythmic delivery of cancer therapeutics. Adv Drug Deliv Rev. 2007;59:1015-35
24. Altinok A, Lévi F, Goldbeter A. Identifying mechanisms of chronotolerance and chronoefficacy for the anticancer drugs 5-fluorouracil and oxaliplatin by computational modeling. Eur J Pharm Sci. 2009;36:20-38
25. Harris BE, Song R, Soong SJ. et al. Relationship between dihydropyrimidine dehydrogenase activity and plasma 5-fluorouracil levels with evidence for circadian variation of enzyme activity and plasma drug levels in cancer patients receiving 5-fluorouracil by protracted continuous infusion. Cancer Res. 1990;50:197-201
26. Zeng ZL, Sun J, Guo L. et al. Circadian rhythm in dihydropyrimidine dehydrogenase activity and reduced glutathione content in peripheral blood of nasopharyngeal carcinoma patients. Chronobiol Int. 2005;22:741-54
Author contact
![]() Corresponding author: Toshiyuki Sakaeda, Ph.D., Center for Integrative Education of Pharmacy Frontier (Frontier Education Center), Graduate School of Pharmaceutical Sciences, Kyoto University 46-29 Yoshidashimoadachi-cho, Sakyo-ku, Kyoto 606-8501, Japan. Tel: +81-75-753-9560, Fax: +81-75-753-4502, E-Mail: sakaedatkyoto-u.ac.jp
Corresponding author: Toshiyuki Sakaeda, Ph.D., Center for Integrative Education of Pharmacy Frontier (Frontier Education Center), Graduate School of Pharmaceutical Sciences, Kyoto University 46-29 Yoshidashimoadachi-cho, Sakyo-ku, Kyoto 606-8501, Japan. Tel: +81-75-753-9560, Fax: +81-75-753-4502, E-Mail: sakaedatkyoto-u.ac.jp
Citation styles
APA
Kuwahara, A., Yamamori, M., Nishiguchi, K., Okuno, T., Chayahara, N., Miki, I., Tamura, T., Kadoyama, K., Inokuma, T., Takemoto, Y., Nakamura, T., Kataoka, K., Sakaeda, T. (2010). Effect of dose-escalation of 5-fluorouracil on circadian variability of its pharmacokinetics in Japanese patients with Stage III/IVa esophageal squamous cell carcinoma. International Journal of Medical Sciences, 7(1), 48-54. https://doi.org/10.7150/ijms.7.48.
ACS
Kuwahara, A.; Yamamori, M.; Nishiguchi, K.; Okuno, T.; Chayahara, N.; Miki, I.; Tamura, T.; Kadoyama, K.; Inokuma, T.; Takemoto, Y.; Nakamura, T.; Kataoka, K.; Sakaeda, T. Effect of dose-escalation of 5-fluorouracil on circadian variability of its pharmacokinetics in Japanese patients with Stage III/IVa esophageal squamous cell carcinoma. Int. J. Med. Sci. 2010, 7 (1), 48-54. DOI: 10.7150/ijms.7.48.
NLM
Kuwahara A, Yamamori M, Nishiguchi K, Okuno T, Chayahara N, Miki I, Tamura T, Kadoyama K, Inokuma T, Takemoto Y, Nakamura T, Kataoka K, Sakaeda T. Effect of dose-escalation of 5-fluorouracil on circadian variability of its pharmacokinetics in Japanese patients with Stage III/IVa esophageal squamous cell carcinoma. Int J Med Sci 2010; 7(1):48-54. doi:10.7150/ijms.7.48. https://www.medsci.org/v07p0048.htm
CSE
Kuwahara A, Yamamori M, Nishiguchi K, Okuno T, Chayahara N, Miki I, Tamura T, Kadoyama K, Inokuma T, Takemoto Y, Nakamura T, Kataoka K, Sakaeda T. 2010. Effect of dose-escalation of 5-fluorouracil on circadian variability of its pharmacokinetics in Japanese patients with Stage III/IVa esophageal squamous cell carcinoma. Int J Med Sci. 7(1):48-54.
This is an open access article distributed under the terms of the Creative Commons Attribution (CC BY-NC) License. See http://ivyspring.com/terms for full terms and conditions.