Impact Factor ISSN: 1449-1907
- Issue 8; 2026
- Issue 7; 2026
- Issue 6; 2026
- Issue 5; 2026
- Issue 4; 2026
- Volume 23; 2026
- Past Issues
- Editorial Board
- Cover Images
- Index & Coverage
- Cover Suggestion
- Special Issues
1. Introduction
2. RNAi Therapeutics Moving from...
3. Risk-Benefit Analysis of RNA...
4. Ethical Analysis
5. Conclusion
References
Footnotes

 Global reach, higher impact
Global reach, higher impactInt J Med Sci 2008; 5(3):159-168. doi:10.7150/ijms.5.159 This issue Cite
Research Paper
Ethical Perspectives on RNA Interference Therapeutics
Mette Ebbesen1, 2, 3, Thomas G. Jensen2, 4, Svend Andersen1, Finn Skou Pedersen3, 5 ![]()
1. Centre for Bioethics and Nanoethics, University of Aarhus, Denmark
2. Faculty of Health Sciences, University of Aarhus, Denmark
3. Interdisciplinary Nanoscience Center (iNANO), University of Aarhus, Denmark
4. Institute of Human Genetics, University of Aarhus, Denmark
5. Department of Molecular Biology, University of Aarhus, Denmark
Received 2008-2-27; Accepted 2008-6-23; Published 2008-6-25
Abstract
RNA interference is a mechanism for controlling normal gene expression which has recently begun to be employed as a potential therapeutic agent for a wide range of disorders, including cancer, infectious diseases and metabolic disorders. Clinical trials with RNA interference have begun. However, challenges such as off-target effects, toxicity and safe delivery methods have to be overcome before RNA interference can be considered as a conventional drug. So, if RNA interference is to be used therapeutically, we should perform a risk-benefit analysis. It is ethically relevant to perform a risk-benefit analysis since ethical obligations about not inflicting harm and promoting good are generally accepted. But the ethical issues in RNA interference therapeutics not only include a risk-benefit analysis, but also considerations about respecting the autonomy of the patient and considerations about justice with regard to the inclusion criteria for participation in clinical trials and health care allocation. RNA interference is considered a new and promising therapeutic approach, but the ethical issues of this method have not been greatly discussed, so this article analyses these issues using the bioethical theory of principles of the American bioethicists, Tom L. Beauchamp and James F. Childress.
Keywords: Ethics, justice, respect for autonomy, risk-benefit analysis, RNA interference therapeutics.
1. Introduction
RNA interference (RNAi) is a specific and efficient natural mechanism for controlling gene expression. In recent years, RNAi has become a powerful tool for probing gene functions and rationalising drug design. It has been employed as a potential therapeutic agent for combating a wide range of disorders, including cancer, infectious diseases and metabolic disorders. A lot of knowledge about RNAi has been accumulated since its discovery in 1998 [1] and findings such as the specific and efficient knock-down of the oncogene K-ras [2] have emphasised the potential of RNAi in clinical applications.
Clinical trials with RNAi have now begun, but major obstacles, such as off-target effects, toxicity and unsafe delivery methods, have to be overcome before RNAi can be considered as a conventional drug. Generally, the success of the therapeutic use of RNAi relies on three conditions: 1) lack of toxicity, 2) specificity of silencing effects and 3) efficacy in vitro and in vivo [3-6]. So if RNAi is to be used therapeutically one should weigh the possible harms against the possible benefits of this method (perform a risk-benefit analysis). The terms harms and benefits are ethically relevant concepts since ethical obligations or principles about not inflicting harm (nonmaleficence) and promoting good (beneficence) are generally accepted [7]. The ethical principles of nonmaleficence and beneficence form part of several different ethical theories. For instance, they are the foundation of the utilitarian theory, which says that ethically right actions are those that favour the greatest good for the greatest number [8]. Another example is the Hippocratic Oath, which expresses an obligation of beneficence and an obligation of nonmaleficence: “I will use treatment to help the sick according to my ability and judgment, but I will never use it to injure or wrong them” [7]. So clearly risk-benefit analysis is an ethical issue. However, according to the American bioethicists Tom L. Beauchamp and James F. Childress [7], ethical issues of biomedicine include not only weighing the possible harms against the possible benefits (risk-benefit analysis), but also considerations about respecting the autonomy of the patient or human subject and considerations about justice with regard to health care allocation. Beauchamp & Childress argue that the four essential ethical principles in biomedicine are the principles of nonmaleficence, beneficence, respect for autonomy and justice. Since RNAi is considered to be a new and promising therapeutic approach, and because the ethical issues of this approach have not been greatly discussed, this article analyses these issues using the ethical principles of Beauchamp & Childress. Firstly, we provide a brief introduction to the RNAi mechanisms and the movement of RNAi from laboratory studies to clinical trials. Secondly, we describe the ethically relevant features of RNAi therapeutics that are important for a risk-benefit analysis. Lastly, we focus on considerations about respecting the autonomy of the patient or human subject and considerations about justice with regard to inclusion criteria for participation in clinical trials and health care allocation.
2. RNAi Therapeutics Moving from Laboratory Studies to Clinical Trials
Background about the RNAi mechanisms
RNAi is a conserved biological mechanism controlling normal gene expression. The silencing mechanisms occur at the levels of transcription, post-transcription and translation. RNAi can also cause augmentation of gene expression due to direct effects on the translation [9]. RNAi is also regarded as a natural defence mechanism against mobile endogenous transposons and invasion by exogenous viruses which have dsRNA as an intermediate product. With this defence mechanism, organisms maintain genetic integrity and hinder infection [10].
Research into RNAi is a fast-developing field and a lot of knowledge has accumulated since its discovery in 1998. In the following, we summarise current knowledge about the RNAi processes.
Post-transcriptional gene silencing
At the initiator step of post-transcriptional gene silencing, long double-stranded RNA (dsRNA), which can be produced by endogenous genes, invading viruses, transposons or experimental transgenes, are cleaved by the enzyme Dicer, which generates 21-23 nucleotide (nt) duplex RNAs with overhanging 3' ends, called small interfering RNAs (siRNAs). Next, siRNAs are incorporated into the RNA-induced silencing complex (RISC), which directs RISC to recognise target mRNAs and cleave them with complementary sequences to the siRNA [11].
Translational gene silencing
RNAi gene inhibition at the level of translation also involves Dicer, which produces 21-to-23-nt-long micro RNAs (miRNAs) synthesised from 60-to-70-nt stem-loop precursor miRNAs (pre-miRNAs). The complex of the activated RISC and miRNA binds the 3'UTR of specific mRNAs, which triggers cleavage by perfect base-pairing recognition or translational repression by partial base-pairing recognition [11].
Transcriptional gene silencing and gene activation
Studies have shown that the RNAi machinery is located in the cytoplasm and therefore acts on mature rather than nuclear precursor mRNA [12]. However, promoter-directed siRNAs can also mediate transcriptional gene silencing in mammalian cells when delivered to the nucleus [13, 14]. This silencing is associated with DNA methylation of the targeted sequence [13, 15]. Moreover, miRNAs complementary to promoter regions have been observed using the RNAi pathway to activate genes in the nucleus [16, 17]. In contrast to silencing, which is triggered within hours and ceases after about seven days, activation takes days to appear but can last for weeks. The mechanism behind this activation is not known.
Pre-clinical studies
Since the obligation not to inflict harm implies an obligation to test a potential drug in animal models before it is delivered to humans, pharmaceutical companies conduct extensive pre-clinical studies. These involve studies in test tubes, cell cultures and animal models to obtain preliminary efficacy, toxicity and pharmacokinetic information and to help decide whether it is worthwhile to go ahead with further testing. Below we present some examples of pre-clinical studies in mouse models to test RNAi against cancer.
Cancer animal models
Animal models are widely used to investigate the therapeutic efficiency of RNAi. In vivo utilisation of siRNA was effectively performed by targeting the colorectal cancer-associated gene beta-catenin. Decreased proliferation and diminished invasiveness were observed following siRNA-mediated silencing of this gene in human colon cancer cells. Additionally, when treated cancer cells were placed in a nude mouse, prolonged survival was seen compared with mice receiving unmanipulated tumours [18]. Similarly, silencing the oncogene H-ras led to inhibition of in vivo tumour growth of human ovarian cancer in a SCID mouse model [19].
To study the effects of inhibition of the oncogenic K-ras expression on the tumourigenic phenotype of human cancer cells, Brummelkamp et al. [2] targeted the expression of the endogenous mutant K-ras V12 allele in a human pancreatic cell line and observed an efficient inhibition of K-ras V12 in the cancer cells. Analysis showed that the siRNAs were sufficiently selective to distinguish between the wild type and the K-ras V12 allele. The oncogenic cells expressing siRNAs against K-ras V12 lost their ability to grow independent of anchorage when plated in semisolid media, and they lost their ability to form tumours in nude mice when transplanted. The experiments performed by Brummelkamp et al. [2] demonstrate that it is possible selectively to knock down just the mutated version of a gene. This gives rise to optimism about the cancer treatment applications of RNAi, for it is possible to design a sequence-specific therapy, which only blocks the expression of an oncogene and not the wild type allele.
Clinical trials for RNAi therapies
Clinical trials with RNAi therapies have already started (Table 1). One of the first applications of RNAi in clinical trials is siRNA for age-related macular degeneration (AMD). AMD is caused by the abnormal growth of blood vessels behind the retina. The treatment strategy is inhibition of the vascular endothelial growth factor pathway by siRNA. These RNAi therapies are designed to be administered directly to the sites of disease in the eye [3]. However, recently new findings call into question the premise behind these clinical trials. Studies in mouse models suggest that the anti-angiogenesis effect is not caused by RNAi, but instead induced in a non-specific manner by RNAs that vary in sequence1 [20].
RNAi based therapies [19].
| Indication | Company | RNAi platform (target) | Clinical stage |
|---|---|---|---|
| Wet AMD | Acuity | Modified siRNA (VEGFR) | Phase II |
| Sirna | Modified siRNA (VEGF) | Phase I/II | |
| Alnylam | siRNA | Phase I | |
| Infectious disease | Alnylam | siRNA for RSV (viral gene) | Phase I |
Clinical trials for RNAi therapies belong to the category of 'treatment trials'2 since new drugs are being tested. Often these trials are designed as randomised, double-blind and placebo-controlled.
Phases
Clinical trials involving new drugs are commonly classified into four phases. Each phase of the drug approval process is treated as a separate clinical trial. The drug-development process will normally proceed through all four phases over many years. If the drug successfully passes through phases I, II and III, it will usually be approved by the national regulatory authority for use in the general population. Phase IV consists of post-approval studies involving the safety surveillance of a drug after it receives marketing approval. The safety surveillance is designed to detect any rare or long-term adverse effects over a much larger patient population and longer time period than was possible during phases I-III clinical trials [21].
Ethical considerations of beneficence and nonmaleficence regarding clinical trials
Generally, participants in a clinical trial benefit from having access to promising new approaches that are often not available outside the clinical trial setting, and they receive regular and careful medical attention from a professional research team. Furthermore, the participants may be the first to benefit from the new method under study. Lastly, the results from the study may help others in the future.
However, participating in a clinical trial also entails some possible risks. For example, new drugs or procedures under study are not always better than the standard care to which they are being compared. The new treatments may have side effects or risks that physicians do not expect or that are worse than those resulting from standard care. Furthermore, participants in randomised trials will not be able to choose the approach they receive and may be required to make more visits to the physician than they would if they were not in the clinical trial [21].
3. Risk-Benefit Analysis of RNA Interference-based Therapies
According to Beauchamp & Childress [22] the evaluation of risk in relation to probable benefit is often labelled risk-benefit analysis. They say that the term risk refers to a possible future harm, where harm is defined as “a setback to interests, particularly in life, health, and welfare” [7]. Statements of risk are both descriptive and evaluative. They are descriptive inasmuch as they state the probability that harmful events will occur, and they are evaluative inasmuch as they attach a value to the occurrence or prevention of the events [7]. In the field of biomedicine, the term benefit commonly refers to something of positive value, such as life or health. The risk-benefit relationship may be conceived in terms of the ratio between the probability and magnitude of an anticipated benefit and the probability and magnitude of an anticipated harm. Use of the terms risk and benefit necessarily involves evaluation. Values determine both what will count as harms and benefits and how much weight particular harms and benefits will have in the risk-benefit calculation [7]. The terms harm and benefit, as defined above, are ethically relevant concepts, since ethical obligations or principles about not inflicting harm (nonmaleficence) and promoting good (beneficence) are generally accepted [7]. According to Beauchamp & Childress [7], the weighing of the general ethical principles of nonmaleficence and beneficence is not symmetrical, since our obligation not to inflict evil or harm (nonmaleficence) is more stringent than our obligation to prevent and remove evil and harm or to do and promote good (beneficence). Our beneficence obligation implies taking action (positive steps) to help prevent harm, remove harm and promote good, whereas our nonmaleficence obligation only implies intentionally refraining from actions that cause harm. So, according to Beauchamp & Childress, possible harms associated with potential therapies are given more weight in a risk-benefit analysis.
To minimise the harm done to patients, medical applications of RNAi require that RNAi is tested in clinical trials, in which the possible risks and possible benefits of potential treatments are evaluated. It is important to identify the ethically relevant features of RNAi which are central for the risk-benefit analysis. These ethical features include siRNA delivery and the specificity of silencing effects.
siRNA Delivery
The challenge of siRNA delivery is to overcome extracellular and intracellular barriers to achieve efficient target cell delivery. Previous studies have shown that siRNA and DNA have difficulty in circulating in the bloodstream, passing across cellular membranes, and escaping from endosomal-lysosomal compartments [23]. Viral and non-viral carrier systems have been developed to increase the delivery of siRNA. For instance, the use of viral vectors based on retrovirus, adenovirus or adeno-associated viruses (AAV) to deliver siRNAs has shown effective gene silencing in vitro and in vivo [24-26]. Below we describe the use of retroviral vectors in more detail.
Retroviral delivery
Retroviruses have some unique properties that make them attractive to biomedical research as tools for gene transfer. Retroviruses are a group of enveloped RNA viruses that replicate via a DNA intermediate that becomes integrated as a provirus into the genome of the host. Integration of the provirus is an advantage, since it results in the stable expression of the genes delivered in the cell and its daughter cells. Using retroviral siRNA expression vectors also allows the addition of regulatory elements to the promoter region so that tissue-specific silencing occurs [27]. Retroviral vectors have been constructed to express siRNAs in order to obtain a persistent gene knock down [2, 28, 29]. However, one of the main drawbacks of retroviral gene therapy trials is insertional mutagenesis. Integrating a retroviral genome into actively transcribed genes and/or protooncogenes may lead to malignancies, as in infants treated for X-linked severe combined immunodeficiency (X-SCID) with retroviral gene therapy [30-32]. But it should be remembered that disease-specific issues may have played an important role in the development of these malignancies. In this specific case, to avoid insertional mutagenesis a small number of cells can be transduced ex vivo and an insertion site analysis performed before they are infused back into the patient. Moreover, when evaluating whether the beneficence of the gene therapy application counterbalances the risks, the severity of the disease should be considered. SCID-X1 is often fatal if not treated, and the only alternative therapy available is unrelated or haploidentical hematopoietic stem cell transplantation, which offers lower correction rates with higher morbidity and mortality than gene therapy [31]. It is generally agreed that the benefits still outweigh the dangers given that there is no known case of vector-triggered cancer other than the SCID-X1 patients [33]. Brummelkamp et al. [2], who have performed specific downregulation of K-ras V12 by retroviral-delivered siRNAs, suggest that “the selective downregulation of only the mutant version of a gene allows for highly specific effects on tumour cells, while leaving the normal cells untouched. This feature greatly reduces the need to design viral vectors with tumour-specific infection and/or expression”. However, when considering the risk of insertional mutagenesis, non-viral delivery systems must also be considered.
Nanoparticle delivery
Non-viral delivery systems, using for instance cationic liposomes and polycation-based carriers such as polyethylenimine (PEI), have been developed for siRNAs. These carriers have been used for in vivo siRNA delivery and gene silencing after intravenous or intranasal administration. However, these systems exhibit in vivo toxicity and activate the immune system [6, 24, 34-37]. This has led to a lot of effort being made to develop efficient carrier materials that are non-toxic, biocompatible and biodegradable. Chitosan, a naturally occurring cationic polysaccharide, is such a material.
Chitosan has been widely used in drug delivery systems, especially for DNA-mediated gene therapy. The positively charged amines of chitosan allow electrostatic interaction with phosphate-bearing nucleic acids to form polyelectrolyte complexes. Furthermore, the protonated amine groups allow transport across cellular membranes and subsequent endocytosis into cells. It has been shown that a chitosan/siRNA nanoparticle delivery system silences genes in vitro and in vivo. Moreover, chitosan has been shown to be biocompatible, non-inflammatory, non-toxic and biodegradable [24]. These facts show the importance of considering chitosan/siRNA nanoparticles as delivery systems in RNAi therapeutics.
Off-target effects
When considering using siRNAs as therapeutic drugs, it is also important to investigate the sequence specificity of RNAi and the risk of off-target effects. For instance, it is vital to ensure that only the targeted mRNA is degraded because otherwise essential genes may be blocked.
It seems that siRNAs can have off-target effects as a result of one of three mechanisms: (1) Since both shRNAs (pre-siRNAs/pre-miRNAs) and siRNAs contain strings of dsRNA, they can activate non-specific cellular innate immune responses such as the interferon response. (2) Transfected or expressed siRNAs might have other non-specific effects. For example, artificial siRNAs or shRNAs could saturate the cell's RNAi machinery and thereby inhibit the function of endogenous miRNAs. (3) Although mature siRNAs are designed to be fully complementary to a single mRNA transcript, they may inadvertently show considerable complementarities to other non-target mRNAs [38].
Interferon response
Studies have shown that an interferon response is induced by dsRNAs more than 30 bp in length, but also perfect dsRNAs as small as 11 bp in length can produce a weak induction [38]. However, steps can be taken to minimise this problem. For instance, since non-specific off-target effects, including activation of the interferon response, are more likely when high levels of an siRNA are used, it is important to transfect the minimum amount of the siRNA duplex that gives rise to a specific RNAi response [39]. It is possible to measure a possible interferon response by analysing the level of expression of an interferon-response gene, such as oligoadenylate synthase-1 (OAS1), by northern-blot or reverse-transcriptase PCR analysis [40, 41].
Saturation of the RNA interference machinery
In addition to the effects of the interferon system, the introduced siRNAs can reportedly saturate the cellular RNAi machinery and thus inhibit the function of endogenous miRNAs and give rise to toxic non-specific effects. These non-specific effects again mandate the use of the lowest effective level of artificial siRNAs in transfection experiments [38].
Changed expression of off-target genes
There are conflicting reports about the specificity of the sequence match between the siRNA and the target mRNA required to achieve specific gene silencing. Elbashir et al. [42] found that a single mismatch between the siRNA and the target mRNA hinders RNAi activity. Contrary to this, Boutla et al. [43] reported that a mutated siRNA with a single centrally located mismatch relative to the mRNA target sequence retained substantial silencing in the fruit fly Drosophila. Studies have shown that siRNAs generally tolerate mutations in the 5'end, while the 3'end exhibits low tolerance [11, 44-47]. These results support the proposed biological function of RNAi as a defence system against viruses, since the tolerance of single mismatches should make viral escape more difficult [44]. The fact that siRNAs are sequence specific to different degrees suggests that the tolerance for mutations is at least partly target-sequence dependent.
If RNAi is used as a therapeutic drug, the above-mentioned studies indicate a need to investigate whether off-target genes with partly sequence similarity to the siRNA also become silenced by the RNAi mechanism. Genes with partly sequence similarity to the siRNA can be found by a BLAST search (NCBI database) against human EST libraries. The monitoring of off-target gene expression must be performed at both the mRNA level and the protein level, making sure that the siRNA does not function as a miRNA and repress translation of off-target mRNAs.
But off-target silencing is not the only thing that needs to be investigated – off-target up-regulations have also been demonstrated. A microarray study by Bakalova [48] shows that silencing one oncogene by RNAi (encoding BCR-ABL fusion protein in chronic myelogenous leukaemia) triggers an overexpression of other 'sleeping' oncogenes, antiapoptotic genes and factors, preserving immortalisation of BCR-ABL-positive leukaemia cells.
Since non-specific off-target effects, including activation of the interferon response and saturation of the RNAi machinery, are more likely when high levels of a siRNA are used, it is important to include an inducible promoter to control the transcription level of siRNAs.
4. Ethical Analysis
The four principles of biomedical ethics
Above, we have described the ethically relevant features of RNAi therapeutics which are important for the risk-benefit analysis. However, according to Beauchamp & Childress [7] ethical issues of biomedicine not only include the balance of the possible harms and the possible benefits (risk-benefit analysis), but also considerations about respecting the autonomy of the patient or human subject and considerations about justice with regard to inclusion criteria for participation in clinical trials and health care allocation. They argue that the four ethical principles of nonmaleficence, beneficence, respect for autonomy and justice are central to and play a vital role in biomedicine. They first published their bioethical theory of principles in 1979, in the book Principles of Biomedical Ethics. This book has been published in many revised and expanded editions [7]. Beauchamp & Childress' bioethical theory is one of the most influential bioethical theories and much research has been carried out by ethicists to reformulate the principles and make them yet more adequate for use in the practice of biomedicine. In Figure 1, we present a brief formulation of the four principles of biomedical ethics.
The four principles of biomedical ethics. A brief formulation of the four bioethical principles of Beauchamp & Childress [7].
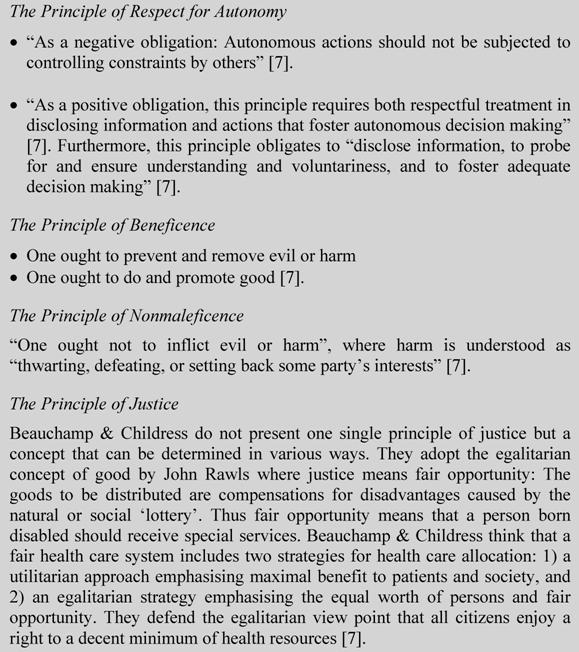
Beauchamp & Childress stress that no one principle ranks higher than the others. Which principles should be given most weight depends on the context of the given situation. Beauchamp & Childress regard the four principles as prima facie binding, i.e. they must be fulfilled, unless they conflict on a particular occasion with an equal principle. Beauchamp & Childress write: “Some acts are at once prima facie wrong and prima facie right, because two or more norms conflict in the circumstances. Agents must then determine what they ought to do by finding an actual or overriding (in contrast to prima facie) obligation” [7]. Thus the agents must find the best balance of right and wrong by determining their actual obligations in such situations through a study of the respective weights of the competing prima facie obligations (the relative weights of all competing prima facie norms) [7].
Beauchamp & Childress [7] believe that the principles find support across different cultures. They claim that the principles are part of a cross-cultural common morality and that in all cultures people who are serious about moral conduct accept the norms of this common morality [7]. But even though these principles are generally acknowledged, this does not mean that there is consensus about what is good and bad. Interesting discussions occur when the principles are to be interpreted, specified and balanced in specific historical, social and political contexts.
Beauchamp [50] claims that the usefulness of the four principles can be tested empirically and that it can be determined whether they are part of a cross-cultural common morality. But he does not present any empirical data to support this position; however, he does invite the design of an empirical research study to investigate the question. A Danish empirical study shows that the four bioethical principles of Beauchamp & Childress are reflected in the daily work of Danish oncology physicians and Danish molecular biologists [51-54].
We have now shown which features of RNAi therapies are important for a risk-benefit analysis. Below, we want to highlight considerations about respect for the autonomy of the patient or human subject and considerations of justice with regard to inclusion criteria for participation in clinical trials and allocation of health care services.
Respect for autonomy
Human subjects agree to participate in clinical trials through informed consent. The information given includes details about standard treatment and about what is involved in the trial, such as the purpose of the study, the tests, and the possible risks and benefits. Subjects or patients can leave the study at any time before the study starts, during the study, or during the follow-up period [21]. The ethical principle governing informed consent is the principle of respect for the autonomy of the human subject or patient. This principle only applies to people able to act autonomously (otherwise they are protected by the principles of nonmaleficence and beneficence) [7]. When analysing the role of the principle of respect for autonomy regarding RNAi gene therapy trials, it is important to consider the risk of generating infection-competent viruses from virus vectors. These replication competent viruses could infect non-consenting people. Furthermore, it is important to consider the risk of introducing genetic changes in germ line cells. This could be seen as tantamount to a clinical experiment on non-consenting subjects belonging to the future generations affected by such changes. Considerations about the risks of generating replication-competent viruses and the risk of introducing genetic changes in germ line cells are also part of risk-benefit analysis.
Justice considerations
Unlike the three other principles, justice is not one single principle, but rather a concept that can be determined in various ways. Consequently, Beauchamp & Childress do not present one principle of justice. Two basic things are more or less given when discussing justice. First, justice – as Aristotle put it – always consists in treating like cases equally. And second, in the context of health care, we are dealing with distributive justice, in which justice is a principle for distributing goods and burdens among individuals in a morally right way. This raises two important questions: What are like cases and what does it mean to treat them equally? And what is a morally right distribution of goods and burdens?
On the latter question, Beauchamp & Childress [7] mention the various answers given by the most prominent theories of justice. These are 1) utilitarianism, which regards justice as the maximisation of utility; 2) libertarianism, in which a just society protects rights of property and liberty and just distribution occurs according to free market forces; 3) egalitarianism, in which inequalities are only allowed if they benefit the least advantaged; and 4) communitarianism, which sees justice determined by the values of a given community. Beauchamp & Childress do not adopt just one of these theories of justice but rather try to combine them. In a way, they treat the theories of justice as they think the four principles should be treated when applied: theories of justice should be specified and balanced with the goal of reaching a coherent health care system.
The various theories of justice differ in defining the good that a health care system distributes. Utilitarianism, of course, regards utility as that good. This is not the view of Beauchamp & Childress – they tend to adopt the egalitarian concept of good in John Rawls' theory of justice. Here, justice means fair opportunity: the goods to be distributed are compensations for disadvantages caused by the natural or social 'lottery'. Thus fair opportunity means that a person born disabled should receive special services, and a child from a poor family should have the same education as other children. Notice, however, that 'same' does not mean 'identical': in the case of education, 'same' means according to intelligence and other properties. In the case of health care 'same' could mean according to need, i.e. to the seriousness and urgency of the suffering [7].
Beauchamp & Childress [7] think that a fair health care system includes two strategies for health care allocation: 1) a utilitarian approach emphasising maximal benefit to patients and society, and 2) an egalitarian strategy that emphasises the equal worth of people and fair opportunity. Beauchamp & Childress defend the egalitarian principle that all citizens have a right to a decent minimum of health resources. This entails a two-tiered system with social coverage for basic and catastrophic health needs, and voluntary private coverage for other health needs, such as better service, luxury hospital rooms, etc. [7].
But the question arises whether people can forfeit this right to a decent minimum of health care. Beauchamp & Childress [7] believe that in some cases people forfeit their right if they are personally responsible for their disease or illness, i.e. if the disease or illness results from personal activities that have been autonomous. They mention several conditions where personal responsibility should affect priorities. One example might be alcoholics who fail to seek effective treatment for alcoholism, suffer from alcohol-related end-stage liver failure, and need liver transplants. And there are several properties for which people are not responsible but which have often served unjustly as bases of distribution; these include gender, race, IQ, and national origin [7]. In contrast, Beauchamp & Childress defend the so-called Fair Opportunity Rule, which says “no persons should receive social benefits on the basis of undeserved advantageous properties (because no persons are responsible for having these properties) and that no persons should be denied social benefits on the basis of undeserved disadvantageous properties (because they also are not responsible for these properties)” [7].
Justice in health care is not, however, restricted to the health care system. It is also connected with rationing and prioritisation (what kinds of health services should be available) and selection (what groups of patients should be eligible for a given service and how to select in individual cases). In relation to these aspects, Beauchamp & Childress also defend a concept of justice that combines equality with utility in the way indicated.
We find Beauchamp & Childress' perception of a fair distribution of healthcare convincing in several ways. However, we presuppose a healthcare system covering in principle all citizens without reference to age, health status, lifestyle, medical condition or employment status. Every person gets national health care, pays no charges for services, is free to choose a provider, and is eligible to receive the services covered, which among others include long-term and chronic care services3. Within this system, excluding people from social coverage because they suffer from a disease caused by personal autonomous activities is seen as unjust. If we now try to apply the principle of justice to RNAi-based treatments, three points are important.
- If these treatments turn out to be medically and economically efficient, there is no doubt that they should be included in the health services accessible to all.
- If we followed Beauchamp & Childress' view on fair distribution of health care, it would be important to ask whether the disease results from personal activities and whether the patient is therefore personally responsible. In some cases, if the person is personally responsible, the treatment should not be covered by the public health care system but by private coverage. Since it is hoped that RNAi-based therapies can cure diverse diseases like cancer, infectious diseases and metabolic disorders, the evaluation of personal responsibility and social coverage of health care needs to be done on a case-by-case basis. For instance, a patient may suffer from a cancer caused by cigarette smoking and seek RNAi therapy to combat this disease. In this case, the patient might be considered personally responsible for the cancer and have to finance the RNAi therapy themselves. However, first of all diseases often result from various factors such as genetic predisposition, personal activities, and social and environmental conditions, and it would be difficult to establish the respective roles of these factors. Secondly, we think it unjust to exclude patients suffering from diseases that they are personally responsible for from the public health care system.
- Justice considerations regarding RNAi therapies are not only important when these therapies are considered as conventional drugs; they are also important during the experimental phase in the development of these therapies. These justice considerations include inclusion criteria for participation in clinical trials. For instance, physicians may justifiably exclude from clinical trials people who suffer from other diseases that might obscure the research result [7]. Until the 1990s, ethical analysis of clinical trials focused on protecting research subjects from harm, abuse and exploitation. The concern was about unfair distribution of burdens. However, in part because of the interest of patients with HIV/AIDS in gaining access to new experimental drugs, the focus shifted during the 1990s towards the benefits of therapeutic trials. As a result, justice in the form of fair access to research became as important as protection from exploitation [7]. This might also be the case with RNAi therapeutics.
5. Conclusion
Research in RNAi therapeutics is a fast developing field and a lot of knowledge about RNAi has accumulated since the mechanisms of RNAi were discovered in 1998. Clinical trials have already begun. We believe it is essential to discuss the ethical issues of RNAi therapies before these therapies are considered as conventional drugs. In this article, therefore, we provided an analysis of the ethically relevant features of RNAi therapies important for a risk-benefit analysis. These ethically relevant features include siRNA delivery and the specificity of silencing effects. For the future development of RNAi-based therapies we believe it is important to perform a risk-benefit analysis and to respect the autonomy of the human subject or patient by considering the risks of generating infection-competent viruses or introducing genetic changes in germ line cells. Furthermore, we think it is important to consider aspects of justice such as equal access vs. private acquisition, and a possible right to participate in clinical trials.
Conflict of interest
The authors have declared that no conflict of interest exists.
References
1. Fire A, Xu S, Montgomery MK, Kostas SA, Driver SE, Mello CC. Potent and specific genetic interference by double-stranded RNA in Caenorhabditis elegans. Nature. 1998;391(6669):806-11
2. Brummelkamp TR, Bernards R, Agami R. Stable suppression of tumorigenicity by virus mediated RNA interference. Cancer Cell. 2002;2(3):243-7
3. Takeshita F, Ochiya T. Therapeutic Potential of RNA Interference against Cancer. Cancer Sci. 2006;97(8):689-696
4. Vorhies JS, Nemunaitis J. Nonviral delivery vehicles for use in short hairpin RNA-based cancer therapies. Expert Rev. Anticancer Ther. 2007;7(3):373-382
5. Kim D, Rossi JJ. Strategies for silencing human disease using RNA interference. Nature Reviews Genetics. 2007;8:173-184
6. Ichim TE, Li M, Qian H, Popov IA, Rycerz K, Zheng XF, White D, Zhong R, Min WP. RNA interference: a potent tool for gene-specific therapeutics. Am J Transplant. 2004;4:1227-1236
7. Beauchamp TL, Childress JF. Principles of biomedical ethics, 6th ed. Oxford: Oxford University Press. 2009
8. Bentham J. An introduction to the principles of morals and legislation (The collected works of Jeremy Bentham). USA: Oxford University Press. 1970
9. Ørom UA, Nielsen FC, Lund AH. MicroRNA-10a binds the 5'UTR of ribosomal protein mRNAs and enhances their translation. Mol Cell. 2008;30(4):460-471
10. Tuschl T. RNA interference and small interfering RNAs. Chembiochem. 2001;2(4):239-45
11. Ma Y, Chan C, He M. RNA interference and antiviral therapy. World J Gastroenterol. 2007;13(39):5169-5179
12. Martinez J, Patkaniowska A, Urlaub H, Lührmann R, Tuschl T. Single-stranded antisense siRNAs guide target RNA cleavage in RNAi. Cell. 2002;110(5):563-74
13. Kawasaki H. siRNA induced transcriptional gene silencing in mammalian cells. Cell Cycle. 2005;4(3):442-448
14. Morris KV. siRNA-mediated transcriptional gene silencing: the potential mechanism and a possible role in the histone code. Cell Mol Life Sci. 2005;62:3057-3066
15. Morris KV, Chan SW, Jacobsen SE, Looney DJ. Small interfering RNA-induced transcriptional gene silencing in human cells. Science. 2004;305:1289-1292
16. Li LC, Okino ST, Zhao H, Pookot D, Place RF, Urakami S, Enokida H, Dahiya R. Small dsRNAs induce transcriptional activation in human cells. Proc Natl Acad Sci USA. 2006;103:17337-17342
17. Check E. Hitting on the switch. Nature. 2007;448(23):855-858
18. Verma UN. Small interfering RNAs directed against beta-catenin inhibit the in vitro and in vivo growth of colon cancer cells. Clin Cancer Res. 2003;9:1291-1300
19. Liu G, Wong-Staal F, Li QX. Development of new RNAi therapeutics. Histol Histopathol. 2007;22:211-217
20. Kleinman ME, Yamada K, Takeda A, Chandrasekaran V, Nozaki M, Baffi JZ, Albuquerque RJC, Yamasaki S. Sequence- and target-independent angiogenesis suppression by siRNA vil TLR3. Nature. 2008;452:591-597
21. US National Institute of Health. National Cancer Institute. http://www.cancer.gov
22. Beauchamp TL, Childress JF. Principles of biomedical ethics. 5th ed. Oxford: Oxford University Press. 2001
23. Pouton CW, Seymour LW. Key issues in non-viral gene delivery. Adv Drug Deliver Rev. 2001;46:187-203
24. Liu X, Howard KA, Dong M, Andersen MØ, Rahbek UL, Johnsen MG, Hansen OC, Besenbacher F, Kjems J. The influence of polymeric properties on chitosan/siRNA nanoparticle formulation and gene silencing. Biomaterials. 2007;28(6):1280-8
25. Xia HB, Mao QW, Paulson HL, Davidson BL. siRNA-mediated gene silencing in vitro and in vivo. Nat Biotechnol. 2002;20:1006-10
26. Barton GM Medzhitov R. Retroviral delivery of small interfering RNA into primary cells. PNAS. 2002;99(23):14943-5
27. Ichim TE, Li M, Qian H, Popov IA, Rycerz K, Zheng X, White D, Zhong R, Min WP. RNA interference: A potent tool for gene-specific therapeutics. Am J Transplant. 2004;4:1227-1236
28. Devroe E, Silver PA. Retrovirus-delivered siRNA. BMC Biotechnol. 2002;2(1):15
29. Paddison PJ, Hannon GJ. RNA interference: the new somatic cell genetics? Cancer Cell. 2002;2(1):17-23
30. Hacein-Bey-Abina S, Von Kalle C, Schmidt M, McCormack MP, Wulffraat N, Leboulch P, Lim A, Osborne CS, Pawliuk R, Morillon E, Sorensen R, Forster A, Fraser P, Cohen JI, de Saint Basile G, Alexander I, Wintergerst U, Frebourg T, Aurias A, Stoppa-Lyonnet D, Romana S, Radford-Weiss I, Gross F, Valensi F, Delabesse E, Macintyre E, Sigaux F, Soulier J, Leiva LE, Wissler M, Prinz C, Rabbitts TH, Le Deist F, Fischer A, Cavazzana-Calvo M. LMO2-associated clonal T cell proliferation in two patients after gene therapy for SCID-X1. Science. 2003;302(5644):415-9
31. Williams DA, Baum C. Gene therapy - new challenges ahead. Science. 2003;302(5644):400-1
32. Racz Z, Hamar P. Can siRNA technology provide the tools for gene therapy of the future? Current Medicinal Chemistry. 2006;13:2299-2307
33. Check E. A tragic setback. Nature. 2002;420(6912):116-8
34. Kawakami S, Hashida M. Targeted delivery systems of small interfering RNA by systemic administration. Drug Metab Pharmacokinet. 2007;22(3):142-151
35. Soutschek J, Akinc A, Bramlage B, Charisse K, Constien RZ, Donoghue M. et al. Therapeutic silencing of an endogenous gene by systemic administration of modified siRNAs. Nature. 2004;432:173-178
36. Schiffelers RM, Ansari A, Xu J, Zhou Q, Tang QQ, Storm G. et al. Cancer siRNA therapy by tumor selective delivery with ligand-targeted sterically stabilized nanoparticle. Nucleic Acids Res. 2004;32(19):e149
37. Bitko V, Musiyenko A, Shulyayeva O, Barik S. Inhibition of respiratory viruses by nasally administered siRNA. Nat Med. 2005;11(1):50-55
38. Cullen RC. Enhancing and confirming the specificity of RNAi experiments. Nature Methods. 2006;3(9):677-681
39. Manche L. Interactions between double-stranded RNA regulators and the protein kinase DAI. Mol Cell Biol. 1992;12:5238-5248
40. Bridge AJ, Pebernard S, Ducraux A, Nicoulaz AL, Iggo R. Induction of an interferon response by RNAi vectors in mammalian cells. Nat Genet. 2003;34:263-264
41. Fish RJ, Kruithof EK. Short-term Cytotoxic Effects and Long-term Instability of RNAi Delivered using Lentiviral Vectors. BMC Mol Biol. 2004;5:9
42. Elbashir SM, Martinez J, Patkaniowska A, Lendeckel W, Tuschl T. Functional anatomy of siRNAs for mediating efficient RNAi in Drosophila melanogaster embryo lysate. EMBO J. 2001;20(23):6877-88
43. Boutla A, Delidakis C, Livadaras I, Tsagris M, Tabler M. Short 5'-phosphorylated double-stranded RNAs induce RNA interference in Drosophila. Curr Biol. 2001;11(22):1776-80
44. Amarzguioui M, Holen T, Babaie E, Prydz H. Tolerance for mutations and chemical modifications in a siRNA. Nucleic Acids Res. 2003;31(2):589-95
45. Jackson AL, Bartz SR, Schelter J, Kobayashi SV, Burchard J, Mao M, Li B, Cavet G, Linsley PS. Expression profiling reveals off-target gene regulation by RNAi. Nat Biotechnol. 2003;21(6):635-7
46. Saxena S, Jónsson ZO, Dutta A. Small RNAs with imperfect match to endogenous mRNA repress translation: Implications for off-target activity of small inhibitory RNA in mammalian cells. J Biol Chem. 2003;278(45):44312-9
47. Chiu YL, Rana TM. siRNA function in RNAi: a chemical modification analysis. RNA. 2003;9(9):1034-48
48. Bakalova R. RNA interference - about the reality to be exploited in cancer therapy Methods Find. Exp Clin Pharmacol. 2007;29(6):417-421
49. Beauchamp TL, Childress JF. Principles of biomedical ethics, 3rd ed. Oxford: Oxford University Press. 1989
50. Beauchamp TL. A defense of the common morality. Kennedy Inst Ethics J. 2003;13(3):259-74
51. Ebbesen M, Pedersen BD. Using empirical research to formulate normative ethical principles in biomedicine. Med Health Care Philos. 2007;10(1):33-48
52. Ebbesen M, Pedersen BD. Empirical investigation of the ethical reasoning of physicians and molecular biologists - the importance of the four principles of biomedical ethics. Philos Ethics Humanit Med. 2007;2:23
53. Ebbesen M, Pedersen BD. The principle of respect for autonomy - concordant with the experience of oncology physicians and molecular biologists in their daily work? BMC Med Ethics. 2008;9:5
54. Ebbesen M, Pedersen BD. The role of ethics in the daily work of oncology physicians and molecular biologists - Results of an empirical study. Business and Professional Ethics Journal. forthcoming
Author contact
![]() Correspondence to: Mette Ebbesen, Centre for Bioethics and Nanoethics, University of Aarhus, Build. 1443, Taasingegade 3, DK-8000 Aarhus C, Denmark. E-mail: mebau.dk Phone: +45 8942 2312
Correspondence to: Mette Ebbesen, Centre for Bioethics and Nanoethics, University of Aarhus, Build. 1443, Taasingegade 3, DK-8000 Aarhus C, Denmark. E-mail: mebau.dk Phone: +45 8942 2312
Footnotes
It may be ethically problematic to continue these trials without reconsiderations, since the basis for the the study and the informed consents given has changed.
Clinical trials are often divided into 1) prevention trials, which test new approaches believed to lower the risk of developing a certain disease, 2) screening trials, which study ways of detecting a certain disease earlier, 3) diagnostic trials, which study tests or procedures that could be used to identify a certain disease more accurately, and 4) treatment trials, which are conducted with patients suffering from a certain disease. They are designed to answer specific questions and evaluate the effectiveness of a new treatment such as a new drug [21].
Beauchamp & Childress [22] suggest the Scandinavian health care systems as ideal way of organising health care delivery in the way indicated. However, these health care systems are currently under pressure and are undergoing a perceptible change. In Denmark, for instance, private hospitals and private health insurances now supplement the public system.