Impact Factor ISSN: 1449-1907

 Global reach, higher impact
Global reach, higher impactInt J Med Sci 2026; 23(7):2376-2386. doi:10.7150/ijms.120352 This issue Cite
Research Paper
Increased Risk of Injury in Patients with Fabry Disease: A Nationwide Population-Based Cohort Study in Taiwan
Chun-Gu Cheng, MD1,2†, Yu-Hsuan Chen, MD3†, Wu-Chien Chien, PhD4,5, Hung-Wen Chiu, PhD6, Fei-Hung Hung, PhD7,8, Hung-Pin Peng, PhD8,9, Chi-Hsiang Chung, PhD4,5, Chun-An Cheng, PhD10 ![]()
1. Department of Emergency Medicine, Taoyuan Armed Forces General Hospital, Taoyuan, Taiwan.
2. Department of Emergency Medicine, Tri-Service General Hospital, National Defense Medical University, Taipei, Taiwan.
3. Department of Chest Medicine, Cheng-Hsin General Hospital, Taipei, Taiwan.
4. School of Public Health, National Defense Medical University, Taipei, Taiwan.
5. Department of Medical Research, Tri-Service General Hospital, National Defense Medical University, Taipei, Taiwan.
6. Graduate Institute of Biomedical Informatics, Taipei Medical University, Taipei, Taiwan.
7. Health Data Analytics and Statistics Center, Office of Data Science, Taipei Medical University, New Taipei City, Taiwan.
8. Research Center of Data Science on Healthcare Industry, College of Management, Taipei Medical University, New Taipei City, Taiwan.
9. Clinical Data Center, Office of Data Science, Taipei Medical University, New Taipei City, Taiwan.
10. Department of Neurology, Tri-Service General Hospital, National Defense Medical University, Taipei, Taiwan.
†These authors contributed equally to this work.
Received 2025-6-26; Accepted 2026-5-9; Published 2026-5-29
Abstract

Background: Fabry disease (FD) is a lysosomal storage disorder leading to α-galactosidase A deficiency and glycosphingolipid accumulation. Neurological manifestations of FD, such as central nervous system involvement, peripheral neuropathy, and vestibular dysfunction that results in postural and cognitive impairment, may predispose individuals to injuries. However, the associations between the risk of injury and FD remains underexplored.
Methods: Using the Taiwanese National Health Insurance Research Database, we conducted a nationwide cohort study of adult FD patients (International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) code 272.7)) who were diagnosed between 2001 and 2015. The comparison group was matched at a 1:4 ratio by age, sex, and index date. Injuries were identified via ICD-9-CM codes 800-999. Multivariate Cox proportional hazards models were applied to study the risk of injury, adjusting for sociodemographic factors and comorbidities.
Results: The injury incidence rate was higher in the FD cohort (32.97/1,000 person-years) than in the control cohort (22.52/1,000 person-years). FD was significantly related to an increased risk of injury (adjusted hazard ratio: 1.642; 95% CI: 1.375-1.980; p < 0.001). FD patients had an 86% greater risk of motor vehicle traffic accidents and a 56% greater risk of falls than the control group. Higher risks of injury were also associated with the winter season, more complicated comorbidities, greater urbanization, and treatment at higher-level hospitals.
Conclusion: This is the first large-scale study to demonstrate a significantly increased risk of injury among FD patients. These findings highlight the need for proactive injury risk assessments and tailored prevention strategies for this population. Future research should investigate the role of FD-related clinical phenotypes in injury susceptibility to enhance personalized care and improve outcomes.
Keywords: injury, Fabry disease, risk
Introduction
Fabry disease (FD) is a rare X-linked lysosomal storage disorder characterized by deficient or absent activity of the enzyme α-galactosidase A (α-Gal A), which reduce the clearance of specific metabolites and thus subsequently cause cellular damage. The accumulation of globotriaosylceramide (Gb3) and related glycosphingolipids throughout the body results in the formation of a cascade of progressive, multisystemic pathologies involving the nervous, cardiovascular, renal, and gastrointestinal systems. Although FD was historically considered to predominantly affect males, it is now well recognized that heterozygous females may also develop significant disease manifestations, often with later onset and greater phenotypic variability [1]. FD affects approximately 1 in 875 males in Taiwan, substantially more than in Western countries [2].
The clinical neurological features of FD, particularly small-fibre neuropathy and central nervous system involvement, result in impaired thermal and pain sensation, proprioceptive deficits, neuropsychiatric disturbances, and vestibular dysfunction [3-5]. These impairments may compromise spatial awareness, motor coordination, and balance, thereby increasing patients' susceptibility to injury [6]. Previous research has largely focused on organ-specific complications in various systems [1], with limited attention given to functional outcomes that may predispose patients to falls, trauma, or other injuries. Moreover, potential differences in injury susceptibility according to sex, disease phenotype, or multisystemic burden remain unclear. To date, no large-scale, population-based studies have investigated the incidence or determinants of injury in FD patients, and evidence-based preventive strategies are lacking.
We conducted a nationwide, population-based cohort study utilizing data from the Taiwan National Health Insurance Research Database to address this critical knowledge gap. Understanding the relationship between FD and the risk of injury is of particular clinical and public health importance in this setting.
We aimed to determine whether FD patients have a greater risk of injury compared to individuals in a matched control population. We hypothesized that FD patients would present a significantly greater incidence of injuries, because of the cumulative effects of multisystemic involvement. However, the common symptoms of FD can involve different types of injuries. Our findings can inform the development of tailored clinical surveillance strategies and preventive interventions to mitigate injury risk in this medically vulnerable population.
Methods
Since 1995, the government in Taiwan has implemented a single-payer National Health Insurance (NHI) program covering all citizens. The Longitudinal Health Insurance Database includes 10% of the population and provides a representative sample of all NHI enrolees in terms of sex, age, and average insurance premiums according to the general population in Taiwan [7]. Deidentified data from databases have been widely used in epidemiological and clinical research by Taiwanese scholars [8].
This study was approved by the Institutional Review Board of TSGHIRB A202305179 and was conducted in accordance with the principles outlined in the Declaration of Helsinki. Given the use of deidentified administrative claims data, the requirement for informed consent was waived.
We identified patients aged 18 years or older who were newly diagnosed with FD between January 2001 and December 2015 according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) code 272.7. Only patients with at least three outpatient visits or hospitalizations associated with the diagnosis of FD were included. Injury-related events were defined using the ICD-9-CM codes 800-999, and follow-up continued through December 31, 2015. A comparison cohort was identified from the remaining dataset of enrolees without any diagnosis of FD. The control group was matched at a 1:4 ratio according to age, sex, and index date to ensure comparability between FD patients and controls. A flowchart of the selection process is shown in Figure 1.
Flowchart of this study.
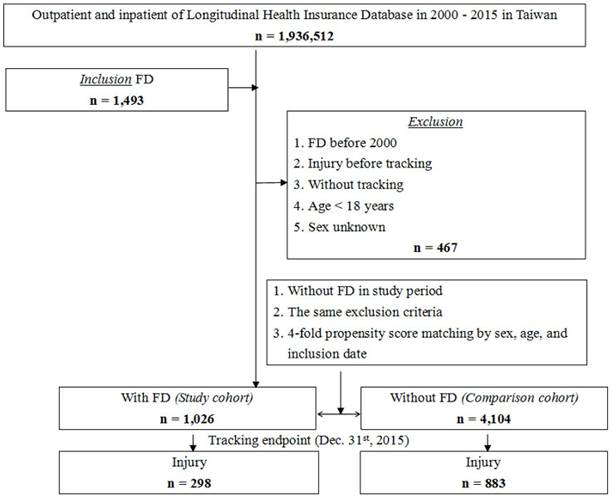
We also examined other possible risk factors, including other medical conditions identified by the ICD-9 CM code. FD patients receiving enzyme replacement treatment were identified on the basis of their prescription records. Additionally, we analysed external cause-of-injury codes (E-codes) to explore the mechanisms of injury. These mechanisms included unintentional injuries such as traffic accidents, poisoning, medically related incidents, falls, burns and fires, drowning, suffocation, crushing injuries, adverse drug reactions, other unintentional injuries), and intentional injuries (including suicide or homicide/abuse) (Table S1 shows the ICD-9-CM codes for comorbidities and the mechanisms of injury.).
The Charlson comorbidity index was revised to exclude hypertension, diabetes mellitus, renal disease, coronary artery disease, cerebrovascular disease, congestive heart failure, alcohol consumption, autoimmune disease, and malignancy (CCI_R).
Descriptive statistics were calculated, and continuous variables were analysed via Student's t test, whereas categorical variables were compared via the chi-square test. Multivariate Cox proportional hazards regression analysis was conducted to evaluate the association between FD and the risk of injury. The model was adjusted for potential confounding variables. The competing risk considered with all-cause mortality of FD was determined by Fine and Gray's competing risk model. Sensitivity analysis was performed by adding 1245 patients (including 249 with FD patients; 996 patients without FD) who experienced injury before tracking. Statistical significance was determined via two-tailed tests with a threshold of p ≤ 0.05. All analyses were performed via SPSS version 21.0.
Results
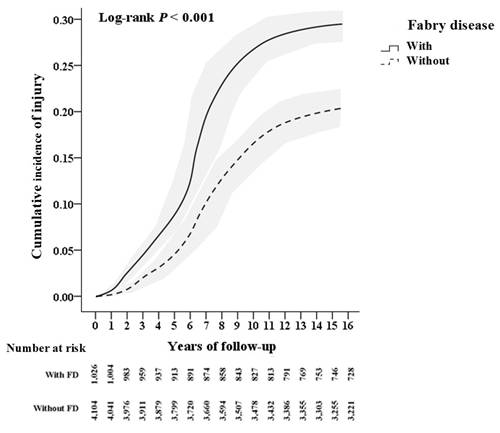
This study included a total of 5,130 participants, comprising 1,026 FD patients and 4,104 matched controls. The incidence of injury was greater in the FD group, with a rate of 32.97 per 1,000 person-years, than in the control group, with a rate of 22.52 per 1,000 person-years, representing an absolute difference of 10.45 per 1,000 person-years (Figure 2). Based on the risk table shown in Figure 2, FD patients who had been diagnosed more than 1 year demonstrated a significantly higher risk of injury.
Kaplan-Meier curve for the cumulative incidence of injury. The patients were stratified on the basis of whether they had or did not have Fabry disease; a log-rank test showed p< 0.001. 1-year adjusted HR: 1.794 (95% CI: 0.762-2.732), p = 0.256. 2-year adjusted HR: 1.583 (95% CI: 1.101-2.248), p <0.001. 3-year adjusted HR: 1.679 (95% CI: 1.265-2.183), p < 0.001. 5-year adjusted HR: 1.657 (95% CI: 1.230-2.175), p < 0.001. > 5-year adjusted HR: 1.640 (95% CI: 1.371-1.976), p < 0.001.
The baseline demographic characteristics and medical comorbidities of FD patients and control participants are summarized in Table 1. The FD patients demonstrated significantly higher rates of anxiety disorders, autoimmune diseases, and hyperthyroidism than the controls. Compared to the main analysis cohort, the sensitivity analysis cohort had a higher proportion of males; a younger mean age; higher rates of hypertension, hyperlipidaemia, depression, and anxiety; a higher proportion of individuals living in middle and eastern Taiwan; lower urbanization; a tendency to visit lower-level hospitals; and lower rates of osteoporosis and malignancy. (Table S2 shows a comparison between the main analysis and sensitivity analysis cohorts).
Baseline characteristics of the study participants.
| Fabry disease (1,026) | No Fabry disease (4,104) | p | SMD | Effect Sizes (Cohen's d) 95%CI | |
|---|---|---|---|---|---|
| Male | 380 (37.04%) | 1,520 (37.04%) | 0.999 | 0.0347 | 0.000 (-0.068, 0.068) |
| Age (years) | 41.18 ± 22.45 | 41.20 ± 22.49 | 0.978 | 0.0349 | -0.001 (-0.069, 0.068) |
| Hypertension | 165 (16.08%) | 633 (15.42%) | 0.603 | 0.0347 | -0.018 (-0.086, 0.050) |
| Diabetes mellitus | 210 (20.47%) | 809 (19.71%) | 0.588 | 0.0349 | -0.019 (-0.087, 0.050) |
| Hyperlipidaemia | 124 (12.09%) | 481 (11.72%) | 0.745 | 0.0349 | -0.011 (-0.080, 0.057) |
| Chronic kidney disease | 139 (13.55%) | 577 (14.06%) | 0.672 | 0.0349 | 0.015 (-0.054, 0.083) |
| Coronary artery disease | 179 (17.45%) | 702 (17.11%) | 0.796 | 0.0347 | -0.009 (-0.077, 0.059) |
| Cerebrovascular disease | 186 (18.13%) | 711 (17.32%) | 0.544 | 0.0347 | -0.021 (-0.089, 0.047) |
| Congestive heart failure | 102 (9.04%) | 365 (8.17%) | 0.342 | 0.0349 | -0.031 (-0.100, 0.037) |
| Depression | 130 (12.67%) | 488 (11.89%) | 0.493 | 0.0349 | -0.024 (-0.092, 0.045) |
| Anxiety | 124 (12.09%) | 325 (7.92%) | < 0.001* | 0.0349 | -0.139 (-0.208, -0.071) |
| Alcohol-related disorder | 223 (21.73%) | 911 (22.20%) | 0.749 | 0.0349 | 0.011 (-0.057, 0.080) |
| Autoimmune disease | 67 (6.53%) | 203 (4.95%) | 0.042* | 0.0349 | -0.068 (-0.137, 0.000) |
| Osteoporosis | 55 (5.36%) | 219 (5.34%) | 0.975 | 0.0347 | -0.001 (-0.069, 0.067) |
| Malignancy | 141 (13.74%) | 578 (14.08%) | 0.778 | 0.0349 | 0.010 (-0.059, 0.078) |
| Migraine | 109 (10.62%) | 412 (10.04%) | 0.579 | 0.0349 | -0.019 (-0.088, 0.049) |
| Hyperthyroidism | 66 (6.43%) | 193 (4.70%) | 0.024* | 0.0349 | -0.076 (-0.144, -0.007) |
| CCI_R | 0.84 ± 1.02 | 0.81 ± 1.00 | 0.392 | 0.0349 | 0.030 (-0.039, 0.098) |
| Season | 0.869 | 0.0349 | -0.028 (-0.096, 0.041) | ||
| Spring (Mar - May) | 265 (25.83%) | 1,011 (24.63%) | |||
| Summer (Jun - Aug) | 281 (27.39%) | 1,125 (27.41%) | |||
| Autumn (Sep - Nov) | 243 (23.68%) | 991 (24.15%) | |||
| Winter (Dec - Feb) | 237 (23.10%) | 977 (23.81%) | |||
| Location | < 0.001* | 0.0352 | -0.456 (-0.525, -0.387) | ||
| Northern Taiwan | 503 (49.03%) | 1,312 (31.97%) | |||
| Middle Taiwan | 262 (25.54%) | 1,017 (24.78%) | |||
| Southern Taiwan | 209 (20.37%) | 1,068 (26.02%) | |||
| Eastern Taiwan | 52 (5.07%) | 513 (12.50%) | |||
| Outlying islands | 0 | 194 (4.73%) | |||
| Urbanization level | < 0.001* | 0.0352 | -0.391 (-0.460, -0.322) | ||
| 1 (The highest) | 351 (34.21%) | 1,084 (26.41%) | |||
| 2 | 482 (46.98%) | 1,316 (32.07%) | |||
| 3 | 77 (7.50%) | 775 (18.88%) | |||
| 4 (The lowest) | 116 (11.31%) | 929 (22.64%) | |||
| Level of healthcare | < 0.001* | 0.0367 | -1.210 (-1.282, -1.138) | ||
| Medical centre | 899 (87.62%) | 1,314 (32.02%) | |||
| Regional hospital | 126 (12.28%) | 1,368 (33.33%) | |||
| Local hospital | 1 (0.10%) | 1,422 (34.65%) |
SMD = standardized mean difference
FD patients had a higher risk of injury than controls with an adjusted hazard ratio (HR) of 1.642 (95% CI: 1.375-1.98; p < 0.001). The adjusted HR of the competing risk model for mortality was1.684 (95% CI: 1.395-2.053; p < 0.001). The risk of injury was also higher in males than in females (adjusted HR: 1.301 (95% CI: 1.145-1.56, p < 0.001)). The risk of injury was also increased in young individuals (adjusted HR:2.03 (95% CI: 1.53-2.514; p < 0.001)) and middle-aged individuals (adjusted HR: 1.835 (95% CI: 1.321-2.308; p < 0.001)) compared to older individuals. Additional increases in the risks of injury were observed in individuals with hypertension (adjusted HR: 1.872 (95% CI: 1.318-2.243; p < 0.001)), diabetes mellitus (adjusted HR: 2.37 (95% CI: 1.682-2.557; p < 0.001)), hyperlipidaemia (adjusted HR: 1.732 (95% CI: 1.24-2.15; p < 0.001)), chronic kidney disease (adjusted HR: 1.685 (95% CI: 1.38-2.301; p < 0.001)), coronary artery disease (adjusted HR: 1.465 (95% CI:1.135-2,101; p < 0.001)), cerebrovascular disease (adjusted HR: 1.503(95% CI: 1.165-2.045; p < 0.001), depression (adjusted HR: 1.774 (95% CI: 1.489-2.056; p < 0.001); anxiety (adjusted HR: 1.732 (95% CI: 1.465-2.001; p < 0.001), alcohol-related disorder (adjusted HR: 2.462 (95% CI: 1.762-3.243; p < 0.001), autoimmune disease (adjusted HR: 1.765 (95% CI.: 1.224-2.508; p < 0.001), osteoporosis (adjusted HR: 1.312 (95% CI: 1.002-1.876; p=0.049), malignancy (adjusted HR: 1.503 (95% CI:1.324-1.98; p < 0.001), and migraine (adjusted HR: 1.264 (95% CI: 1.098-1.486; p = 0.002). The CCI_R was associated with injury with an adjusted HR of 1.165 (95% CI: 1.086-1.27; p = 0.007). Compared with spring, winter was associated with a greater risk of injuries, with an adjusted HR of 1.465 (95% CI: 1.113-1.774; p < 0.001) being reported. Higher urbanization level was associated with a greater risk of injury than the lowest urbanization level. Patients who visited medical centres exhibited a greater risk, with an adjusted HR 1.876 (95% CI: 1.444-2.223; p < 0.001) being observed; moreover, those who visited regional hospitals demonstrated a greater risk of injury with an adjusted HR 1.68 (95% CI: 1.206-2.01; p < 0.001) being observed than those who visited local hospitals. Sensitivity analysis revealed that FD was associated with the risk of injury with an adjusted HR of 1.689 (95% CI: 1.437-2.036; p < 0.001) (Table 2).
Risk factors for injury according to Cox regression.
| Variables | Adjusted hazard ratio | p |
|---|---|---|
| Fabry disease | ||
| Non-competing risk model | 1.642(95% CI:1.375-1.980) | < 0.001* |
| Competing risk model | 1.684 (95% CI: 1.395-2.053) | < 0.001* |
| Sensitivity analysis | 1.689 (95% CI: 1.437-2.036) | < 0.001* |
| Male | 1.301 (95% CI: 1.145-1.560) | < 0.001* |
| Age group | ||
| Young | 2.03 (95% CI: 1.53-2.514) | < 0.001* |
| Middle-aged | 1.835 (95% CI: 1.321-2.038) | < 0.001* |
| Older | Reference | |
| Hypertension | 1.872 (95% CI: 1.318-2.243) | < 0.001* |
| Diabetes mellitus | 2.37 (95% CI: 1.682-2.557) | < 0.001* |
| Hyperlipidaemia | 1.732 (95% CI: 1.24-2.15) | < 0.001* |
| Chronic kidney disease | 1.685 (95% CI: 1.38-2.301) | < 0.001* |
| Coronary artery disease | 1.465 (95% CI: 1.135-2.101) | < 0.001* |
| Cerebrovascular disease | 1.503(95% CI: 1.165-2.045) | < 0.001* |
| Congestive heart failure | 1.432 (95% CI: 0.998-2.713) | 0.052 |
| Depression | 1.774 (95% CI: 1.489-2.056) | < 0.001* |
| Anxiety | 1.732 (95% CI: 1.465-2.001) | < 0.001* |
| Alcohol-related disorder | 2.462 (95% CI: 1.762-3.243) | < 0.001* |
| Autoimmune disease | 1.765 (95% CI: 1.224-2.508) | < 0.001* |
| Osteoporosis | 1.312 (95% CI: 1.002-1.876) | 0.049* |
| Malignancy | 1.503 (95% CI:1.324-1.98) | < 0.001* |
| Migraine | 1.264 (95% CI: 1.098-1.486) | 0.002* |
| Hyperthyroidism | 1.087 (95% CI: 0.865-1.271) | 0.145 |
| CCI_R | 1.165 (95% CI: 1.086-1.27) | 0.007* |
| Season | ||
| Spring | Reference | |
| Summer | 1.065 (95% CI: 0.725-1.33) | 0.259 |
| Autumn | 1.267 (95% CI: 0.973-1.589) | 0.077 |
| Winter | 1.465 (95% CI: 1.113-1.774) | < 0.001* |
| Urbanization level | ||
| 1 (The highest) | 1.597 (95% CI: 1.331-1.806) | < 0.001* |
| 2 | 1.552 (95% CI: 1.328-1.794) | < 0.001* |
| 3 | 1.303 (95% CI: 1.114-1.52) | < 0.001* |
| 4 (The lowest) | Reference | |
| Level of healthcare | ||
| Medical centre | 1.876 (95% CI: 1.444-2.223) | < 0.001* |
| Regional hospital | 1.68 (95% CI: 1.206-2.01) | < 0.001* |
| Local hospital | Reference |
CI: confidence interval; CCI_R: Charlson comorbidity index revised to exclude hypertension, diabetes mellitus, chronic kidney disease, coronary artery disease, cerebrovascular disease, congestive heart failure, alcohol consumption, autoimmune disease, and malignancy. Sensitivity analysis included patients with a previous history of injury (Fabry disease, n = 249; no Fabry disease, n = 996)
Stratified analyses demonstrated that, across all of the subgroups defined by age, sex, comorbidity burden, season, and urbanization level, FD was consistently associated with a significantly increased risk of subsequent injury. This association remained particularly pronounced among patients treated at medical centres and regional hospitals, where FD patients exhibited substantially higher injury risks than non-FD individuals did (Table S3 shows stratified analyses across all the subgroups). FD Patients were further stratified by clinical manifestations and treatment modalities, after which they were compared with non-FD patients. Those who presented with neuropathic symptoms, hypotension, syncope, sleep disorders, anaemia, and peripheral vertigo; those who were hospitalized; those who received enzyme replacement treatment; and those underwent rehabilitation demonstrated a markedly increased risk of injury. A longer duration of hospitalization was associated with a higher risk of injury. A longer duration of enzyme replacement treatment demonstrated lower risk of injury trend (Table S4 shows analyses stratified by clinical manifestations and treatment modalities, comparing individuals with and without FD). In terms of the different injury types, FD patients had increased risks of motor vehicle collision (HR: 1.863 (95% CI: 1.552-2.247, p < 0.001)), poisoning (HR: 2.207 (95% CI: 1.849-2.669, p < 0.001)), falls (HR: 1.56 (95% CI: 1.305-1.883, p < 0.001)), burns (HR: 1.213 (95% CI: 1.03-1.467, p = 0.035)), suffocation (HR: 1.46 (95% CI: 1.221-1.763, p < 0.001), crushing injuries (HR: 1.328 (95% CI: 1.11-1.604, p < 0.001)) and injuries caused by animals (HR: 1.217 (95% CI: 1.018-1.469, p = 0.041)). The severity of injuries was classified by using the injury severity score (ISS). The results demonstrated that major trauma (ISS ≥ 16) exhibited an adjusted HR of 2.018 (95% CI:1.69-2.434, p < 0.001), moderate trauma (ISS: 9-15) exhibited an adjusted HR of 1.958 (95% CI:1.64-2.361, p < 0.001) and minor trauma (ISS ≤ 8) exhibited an adjusted HR of 1.386 (95% CI: 1.161-1.671, p < 0.001). The more severe injuries demonstrated higher risks regarding traffic accidents, poisoning and fall (Table 3). A cross table of the different types of injuries and comorbid conditions was constructed (Table S5 shows the distribution of Fabry disease patients according to their comorbidities and causes of injury). Among individuals with FD-related neuropathy, 34.16% of traffic accidents and 14.29% of fall incidents were attributable to neuropathic manifestations. Among individuals with a history of stroke, 22.41% were involved in traffic accidents, and 15.52% experienced falls. Among individuals with a history of congestive heart failure, 25% experienced falls and traffic accidents. Among individuals with a history of coronary artery disease, 24.56% experienced traffic accidents, and 17.54% experienced falls. Among individuals with a history of peripheral vertigo, 19.05% experienced falls and traffic accidents. Among individuals with a history of hypotension, 32.65% experienced traffic accidents, and 24.49% experienced falls. Among individuals with a history of chronic kidney disease, 20.63% were involved in traffic accidents, and 11.11% experienced falls. However, among individuals with a history of sedation treatment, 17.33% were involved in traffic accidents and 13.33% experienced falls. The proportion of poisoning events was elevated among individuals receiving treatment for congestive heart failure (18/75%), sedation treatment (18.67%), neuropathy treatment (18.63%), and enzyme replacement therapy (12.36%).
Risk of injury subgroups by Cox regression
| Fabry disease | With | Without (reference) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Injury subgroups | Events | PYs | Rate | Events | PYs | Rate | aHR (95% CI) | p | Related conditions |
| Overall | 298 | 9,039.08 | 32.97 | 883 | 39,201.92 | 22.52 | 1.642 (1.375-1.980) | < 0.001* | |
| Unintentional injury | 246 | 9,039.08 | 27.22 | 681 | 39,201.92 | 17.37 | 1.758 (1.47-2.124) | < 0.001* | |
| Traffic injuries | 132 | 9,039.08 | 14.60 | 345 | 39,201.92 | 8.80 | 1.863 (1.552-2.247) | < 0.001* | N, ERT, Hypo, CAD |
| Major trauma (ISS≥ 16) | 26 | 9,039.08 | 2.88 | 53 | 39,201.92 | 1.35 | 2.387 (1.999-2.878) | < 0.001* | |
| Moderate trauma (ISS: 9 - 15) | 44 | 9,039.08 | 4.87 | 96 | 39,201.92 | 2.45 | 2.230 (1.867-2.691) | < 0.001* | |
| Minor trauma (ISS ≤ 8) | 62 | 9,039.08 | 6.86 | 196 | 39,201.92 | 5.00 | 1.539 (1.273-1.857) | < 0.001* | |
| Poisoning | 39 | 9,039.08 | 4.31 | 86 | 39,201.92 | 2.19 | 2.207 (1.849-2.669) | < 0.001* | N, Sed, ERT |
| Major trauma (ISS≥ 16) | 9 | 9,039.08 | 1.00 | 16 | 39,201.92 | 0.41 | 2.994 (2.503-3.612) | < 0.001* | |
| Moderate trauma (ISS: 9 - 15) | 13 | 9,039.08 | 1.44 | 27 | 39,201.92 | 0.69 | 2.435 (2.035-2.939) | < 0.001* | |
| Minor trauma (ISS ≤ 8) | 17 | 9,039.08 | 1.88 | 43 | 39,201.92 | 1.10 | 1.888 (1.582-2.271) | < 0.001* | |
| Falls | 43 | 9,039.08 | 4.76 | 134 | 39,201.92 | 3.42 | 1.56 (1.305-1.883) | < 0.001* | N, ERT, Hypo, Sed, CAD, Stroke |
| Major trauma (ISS≥ 16) | 10 | 9,039.08 | 1.11 | 29 | 39,201.92 | 0.74 | 1.946 (1.631-2.348) | < 0.001* | |
| Moderate trauma (ISS: 9 - 15) | 15 | 9,039.08 | 1.66 | 44 | 39,201.92 | 1.12 | 1.840 (1.541-2.220) | < 0.001* | |
| Minor trauma (ISS≤ 8) | 18 | 9,039.08 | 1.99 | 61 | 39,201.92 | 1.56 | 1.327 (1.112-1.607) | < 0.001* | |
| Burns and fires | 3 | 9,039.08 | 0.33 | 12 | 39,201.92 | 0.31 | 1.213 (1.03-1.467) | 0.035* | N, Stroke, CKD |
| Drowning | 2 | 9,039.08 | 0.22 | 9 | 39,201.92 | 0.23 | 1.083 (0.905-1.306) | 0.118 | |
| Suffocation | 9 | 9,039.08 | 1.00 | 30 | 39,201.92 | 0.77 | 1.46 (1.221-1.763) | < 0.001* | Sed, CHF,PV |
| Crushing / cutting / piercing | 6 | 9,039.08 | 0.66 | 22 | 39,201.92 | 0.56 | 1.328 (1.11-1.604) | < 0.001* | ERT, CKD, Sed, CAD, Hypo |
| Excessive heat | 0 | 9,039.08 | 0.00 | 1 | 39,201.92 | 0.03 | 0 | 0.999 | |
| Injury caused by animal | 1 | 9,039.08 | 0.11 | 4 | 39,201.92 | 0.10 | 1.217 (1.018-1.469) | 0.041* | N, Stroke, CKD |
| Electric current injury | 0 | 9,039.08 | 0.00 | 2 | 39,201.92 | 0.05 | 0 | 0.999 | |
| Other unintentional injuries | 11 | 9,039.08 | 1.22 | 36 | 39,201.92 | 0.92 | 1.483 (1.241-1.792) | < 0.001* | |
| Intentional injury | 23 | 9,039.08 | 2.54 | 101 | 39,201.92 | 2.58 | 1.108 (0.925-1.337) | 0.104 | |
| Suicide | 13 | 9,039.08 | 1.44 | 59 | 39,201.92 | 1.51 | 1.071 (0.896-1.29) | 0.139 | |
| Homicide / abuse | 10 | 9,039.08 | 1.11 | 42 | 39,201.92 | 1.07 | 1.159 (0.97-1.398) | 0.073 | |
| Intention unknown | 5 | 9,039.08 | 0.55 | 18 | 39,201.92 | 0.46 | 1.352 (1.134-1.622) | < 0.001* | |
| Without E-code | 24 | 9,039.08 | 2.66 | 83 | 39,201.92 | 2.12 | 1.413 (1.182-1.705) | < 0.001* | |
| Major trauma (ISS≥ 16) | 56 | 9,039.08 | 6.20 | 135 | 39,201.92 | 3.44 | 2.018 (1.69-2.434) | < 0.001* | |
| Moderate trauma (ISS: 9 - 15) | 99 | 9,039.08 | 10.95 | 246 | 39,201.92 | 6.28 | 1.958 (1.64-2.361) | < 0.001* | |
| Minor trauma (ISS≤ 8) | 143 | 9,039.08 | 15.82 | 502 | 39,201.92 | 12.81 | 1.386 (1.161-1.671) | < 0.001* | |
*p<0.05; PYs: person-years; rate: per 1,000 PYs; CI: confidence interval; ISS: injury severity score; aHR: adjusted hazard ratio, adjusted for the variables listed in Table 2.; N: neuropathy; Hypo: hypotension; CAD: coronary artery disease; Sed: sedation treatment; CKD: chronic kidney disease; CHF: congestive heart failure; PV: peripheral vertigo
Discussion
This is the first epidemiological study to compare the incidence of injury between individuals with and without FD. Our findings revealed a significant association between FD and a 64% increase in the risk of injury. FD patients demonstrated an 86% greater risk of motor vehicle traffic accidents and a 56% greater risk of falls than matched controls.
Neuropathy in FD
In FD, male patients tend to present with symptoms earlier than female patients do. Neurological involvement generally manifests around adolescence, followed by cardiac features and renal complications at thirty years of age [9]. The underlying pathophysiology is thought to involve Gb3 accumulation in neural structures, including the perineurium, the endothelial cells of the vasa nervorum, the dorsal root ganglia, and the Schwann cells. Neuropathic pain predominantly affects the distal extremities and is characterized by diminished thermal sensation, burning dysaesthesias, and episodic pain crises that significantly impair quality of life and may alter gait patterns with a concomitant reduction in proprioception [3,10-11]. Such neuromotor instability markedly increases the risk of falls and impairs limb coordination, and early physiotherapy is needed. FD patients exhibit increased risk of for various types of injury, primarily due to the fact that the sensory neuropathy resulting from the disease leads to impaired perception (especially in the extremities), thereby increasing the likelihood of burns and cuts from unnoticed contact with hot or sharp objects [10].
Cognitive function in FD
Central nerve system involvement is well documented in FD patients [3]. Imaging studies have demonstrated altered connectivity within the motor cortex and microstructural abnormalities in the thalamus, potentially implicating disrupted motor control pathways. Cerebellar involvement has also been reported [12]. Changes in white matter are common in FD-related cognitive impairment [13,14]. Emerging evidence has also linked FD to parkinsonian features with postural instability [15,16]. Additionally, neuropsychiatric manifestations, including depression and anxiety, are common and may exacerbate the decline in cognitive function in FD patients [17], potentially increasing the incidence of injury. It might be beneficial to encourage aerobic exercise, mindfulness, and cognitive training to improve executive activity for driving and other daily activities. Furthermore, sedation treatment is associated with a reduced risk of injury.
Stroke in FD
In lysosomal storage disorders such as FD, persistent antigenic stimulation perpetuates inflammatory signalling, rendering inflammation a chronic process [18]. The pathological accumulation of Gb3 substrates within vascular endothelial cells is a hallmark feature of FD [19]. This glycosphingolipid-induced vasculopathy disrupts normal vascular function, leading to impaired perfusion across multiple organ systems, including the renal, cardiac, central nervous, and peripheral nervous systems. In FD, the intima thickness increases, and flow-mediated dilation decreases [19]. Reduced cerebral blood flow and cerebrovascular autoregulation impairment were noted in FD [20]. An increased incidence of stroke in FD in the United States has been reported [21]. FD is common in patients with cryptogenic stroke who present with proteinuria and basilar artery involvement [22]. In Asian stroke populations, the prevalence of FD is approximately 0.62% according to the Fabry Outcome Survey, with male patients typically being affected at a younger age [23]. Patients who have had a stroke present impaired cognitive function [24] and motor coordination. Consistent physiotherapy is needed to address for balance impairment and limb weakness. FD patients with comorbid stroke, neuropathy or chronic kidney disease were observed to have slower processing speed, and executive dysfunction, which can increase susceptibility to animal-related injuries. The caregivers of such patients need to prevent animal attacks.
Cardiovascular conditions in FD
Lysosomal dysfunction in FD is related to impaired mitochondrial function and impaired cardiac energy metabolism [25]. Gb3 accumulation promotes inflammation and fibrotic cascades in various tissues, including the myocardium, where it contributes to arrhythmias, left ventricular hypertrophy, interventricular septal thickening, myocardial fibrosis, and hypoxia. Additionally, mild to moderate valvular heart disease, particularly mitral and aortic valve thickening with mild regurgitation, is frequently observed [26, 27]. Cardiac problems can increase falls [28]. In patients with congestive heart failure, driving performance is reduced [29]. Cardiovascular events can lead to symptoms such as dizziness, syncope, and cerebral hypoperfusion, all of which can impair driving performance [30].
Chronic kidney disease in FD
Gb3 accumulation in the podocytes of the glomeruli within the nephrons results in fibrosis, tubular atrophy, and chronic kidney disease. Symptoms of FD include the involvement of various organ systems as a result of the accumulation of Gb3 in endothelial cells, initiating a downstream cascade of events leading to inflammation and organ damage [31]. One-fifth of FD patients with chronic kidney disease experienced traffic accidents. Renal function impairment needs to be improved through treatment. Anaemia is common in FD patients, and its prevalence is strongly associated with declining renal function, the presence of heart failure and chronic inflammation. Anaemia may decrease the oxygen supply, resulting in impaired physical endurance and cognitive alertness, which may indirectly increase the risk of injury in this population [32]. FD patients with anaemia demonstrate a higher risk of injury than those without anaemia. The cause of anaemia needs to be corrected as soon as possible.
Dizziness in FD
Approximately eighty percent of FD patients reported problems of dizziness or balance. [5]. Tinnitus is significantly more prevalent in individuals with FD, with an adjusted odds ratio of 1.5, than in the general population [33]. The underlying pathophysiology may involve cochleovestibular ischaemia secondary to endothelial Gb3 accumulation. Persistent vestibular deficits may lead to spatial disorientation in FD patients, particularly during high-speed or curved motion [34], and these deficits can significantly impair postural control which is a function that is reliant on integrated visual, vestibular, and proprioceptive input [6]. Among FD patients in China, 80% exhibit oculomotor problems and 40% demonstrate vestibulo-oculomotor dysfunctions [35]. These impairments increase susceptibility to falls, traffic accidents, and injury and are often associated with psychological comorbidities such as anxiety and social withdrawal. Among individuals with a history of peripheral vertigo, one-fifth experienced falls or traffic accidents. Moreover, these individuals have required vestibular rehabilitation. Autonomic neuropathy is a recognized manifestation of FD and may contribute significantly to orthostatic hypotension, which presents as dizziness, lightheadedness, or syncope [36]. Among FD patients with hypotension as a complication found one-third experienced traffic accidents and one-quarter experienced falls. Regular blood pressure checks are recommended, hypotension must be treated with inotropic agent.
Sleep problems in FD
Approximately 65% of FD patients report of experiencing sleep disturbances, with a slightly higher prevalence among females. Excessive daytime sleepiness is disproportionately common in FD patients and may contribute to an increased risk of injury. In addition, the prevalence of obstructive and central sleep apnoea in FD patients appears comparable to that in the general population [37]. Patients who have sleep problems associated with an increased risk of injury can reduce this risk by receiving sedation treatment to improve their sleep problems. Autonomic or central involvement can cause gastrointestinal dysmotility and, in severe cases, dysphagia, which may increase the risk of aspiration and suffocation [38,39].
Other comorbidities of FD
Patients with diabetes mellitus have an increased rate of motor vehicle accidents [40]. Our findings demonstrated that comorbidities, such as hypertension, hyperlipidaemia, and diabetes mellitus, are associated with an increased risk of injury. Fatigue and exercise intolerance are common symptoms caused by to cardiac and pulmonary dysfunctions in FD patients [41,42]. Consistent with the findings of previous studies in young adults, alcohol-related disorders were associated with a significantly increased risk of injury [43]. Migraines (which are characterized by photophobia, altered sensory processing, and central nerve system dysfunction) are known to impair driving performance with an HR of 1.78 being reported for traumatic head injury [44,45] and an odds ratio of 3.3 being reported for motor vehicle collisions within one year [46]. In our study, alcohol-related disorders caused by complications related to the alcohol consumption were associated with an increased risk of injury. Moreover, exposure to low ambient temperatures has been shown to increase the risk of falls [47]. Consistent with these findings, our study revealed an increased risk of injury during the winter.
Treatment of FD
In Taiwan, enzyme replacement treatment and pharmacological chaperones are covered by health insurance but require rigorous clinical documentation and approval, including evidence of characteristic symptoms (e.g., small-fibre neuropathy, left ventricular hypertrophy, and proteinuria) and, in some cases, pathological confirmation via biopsy [48]. Treatment helps mitigate symptoms and improve quality of life but cannot provide a cure [49]. FD patients who received enzyme replacement treatment tended to have more severe symptoms and a greater risk of injury than those who did not receive treatment. Impaired renal and hepatic function further predisposes FD patients to drug toxicity and poisoning; however, adverse reactions to enzyme replacement therapy may temporarily reduce physical or cognitive alertness [17]. An increased proportion of poisoning events were observed among FD patients receiving treatment for congestive heart failure, as well as sedation treatment, neuropathy treatment, and enzyme replacement therapy. Before treatment, renal and hepatic function need to be checked. Adjunctive rehabilitation strategies tailored to FD patients may further support balance, coordination, and mobility [50], but FD patients seem to have an increased risk of injury, potentially because of delayed interventions.
Risk regarding short duration of FD and small cells of different type injuries
The non-significant hazard ratio observed at the 1-year follow-up (p = 0.256) may indicate that injury risk in patients with FD progressively accumulates with disease advancement. During the early stages, subclinical organ involvement and compensatory physiological mechanisms may mitigate overt clinical manifestations, thereby attenuating detectable risk and diluting short-term effect estimates. These findings underscore the importance of longitudinal evaluation and suggest that extended follow-up is necessary to more accurately delineate the dynamic and evolving risk profile associated with FD. The distribution of patients with FD across comorbid conditions revealed extremely sparse event counts in certain categories, including burns (n = 3), animal-related injuries (n = 1), and cutting/piercing injuries (n = 6). Given the limited number of cases detected in these subgroups, these observations should be interpreted with caution. Accordingly, the analyses pertaining to these categories are considered to be exploratory in nature to avoid over-interpretation.
The strengths of this study include the use of a large, nationwide population-based dataset. The inclusion of individuals who participate in Taiwan's universal health insurance system (which is characterized by low copayments and comprehensive coverage) minimized selection bias. The increased injury risk in FD has implications for healthcare utilization, disability prevention, and resource allocation, potentially leading to hospitalization, prolonged rehabilitation, and a socioeconomic burden. Additionally, the NHI claims data capture all healthcare utilization events for FD patients and injuries across the entire population, reducing the recall bias inherent in self-reported data. The genetic diagnosis of FD was partially funded by the Rare Disease Foundation in Taiwan, and treatment is fully covered by Taiwan's single-payer health insurance, reducing the financial burden and ensuring timely medical care. With highly accessible healthcare, patients who experience injuries can receive timely medical assistance. Annual evaluations should assess visual, auditory, cognitive, and motor functions, and driving should be discouraged to reduce the risk of accidents when deficits are detected. Early identification of high-risk individuals could enable timely interventions. It is recommended that FD patients undergo a 10-metre walk test every year, and those with a reduced gait speed < 0.8 metre/second should receive a walking aid and early physiotherapy to prevent falls [51, 52]. FD patients are recommended to undergo a clock drawing test to evaluate their cognitive activity, executive activity and hand coordination. Clinicians should advise neuropathic pain management, vestibular rehabilitation, and avoidance of high-risk activities. Enhancing awareness among caregivers, employers, social services, and public health agencies is essential for creating safer environments and reducing injury-related morbidity. These findings underscore the need for multidisciplinary approaches involving neurology, rehabilitation, cardiology, and public health professionals.
Limitations
Several limitations of this study should be acknowledged. First, the dataset lacked information on disease severity, genetic variants, laboratory parameters (such as nerve conduction study, echocardiography, renal function test, and haemoglobin test results), anthropometric data (such as height and weight), and lifestyle factors, including smoking and alcohol consumption (all of which may influence gait stability and injury risk). Registry studies can overcome this limitation. Second, the administrative claims data did not capture detailed information of the severity of nerve injury, renal function, and cardiac function regarding the mechanisms, thereby limiting the granularity of injury characterization and precluding a full understanding of the injury spectrum in FD patients. The integration of richer clinical datasets and the inclusion of family members or healthcare providers are needed to enhance the comprehensiveness of FD risk profiling and injury prevention strategies. Third, although comorbidities were observed to be associated with increases in FD patients' rates of higher traffic accidents, falls and poisoning events, the cause-effect relationship could not be established in this study. Future studies must be designed to survey the actual risk. Fourth, the generalizability of our findings is limited, as the majority of participants were of Han Chinese ethnicity. The clinical burden of FD in Taiwan is thus disproportionately high and warrants targeted public health and clinical research efforts [2]. The support of the national health insurance system ensured access to high-quality care while minimizing the economic burden on patients. Injured patients received better care because of improved access to healthcare services. Medical centres specializing in FD provided professional diagnosis and comprehensive care, including genetic screening for family members, which facilitated early detection. Future research should aim to incorporate more diverse populations and healthcare systems. Fifth, our incidence information was derived from the injury codes included in the claim dataset; thus, some minor injuries that were resolved without outpatient or inpatient visits may have gone unreported, thereby causing the incidence of injury to be underestimated.
Conclusion
This study revealed a significantly increased risk of injuries among FD patients. The progressive multisystem involvement characteristic of FD may contribute to impaired gait stability, altered cognitive function, and reduced execution, all of which predispose patients to accidental harm. Given these findings, clinicians should remain vigilant in monitoring the evolving clinical course of FD and proactively assessing injury risk. Moreover, caregivers should provide appropriate support in daily activities to help mitigate the occurrence of injuries in this vulnerable population.
Supplementary Material
Supplementary tables.
Acknowledgements
The authors are thankful for the support received by grant from the Taoyuan Armed Forces General Hospital TYAFGH-E-115048 and from the Cheng Hsin General Hospital CHGH115-N01 for this study.
Competing Interests
The authors have declared that no competing interest exists.
References
1. Thompson SE, Roy A, Geberhiwot T. et al. Fabry Disease: Insights into Pathophysiology and Novel Therapeutic Strategies. Biomedicines. 2025;13:624 doi: 10.3390/biomedicines13030624
2. Hwu WL. Deciphering the diagnostic dilemma: A comprehensive review of the Taiwanese cardiac variant in Fabry disease. J Formos Med Assoc. 2024;123:738-743 doi: 10.1016/j.jfma.2023.10.004
3. Tuttolomondo A, Baglio I, Riolo R. et al. Molecular Pathogenesis of Central and Peripheral Nervous System Complications in Anderson-Fabry Disease. Int J Mol Sci. 2023;25:61 doi: 10.3390/ijms25010061
4. Bolsover FE, Murphy E, Cipolotti L. et al. Cognitive dysfunction and depression in Fabry disease: a systematic review. J Inherit Metab Dis. 2014Mar;37(2):177-87 doi: 10.1007/s10545-013-9643-x
5. Johansen AB, Feldt-Rasmussen U, Klokker M. Dizziness in Fabry Disease. Biomedicines. 2025;13:249 doi: 10.3390/biomedicines13020249
6. Peultier-Celli L, Jaussaud R, Kaminsky P. et al. Balance control impairments in Fabry disease. Front Neurol. 2022;13:856946 doi: 10.3389/fneur.2022.856946
7. Ministry of Health and Welfare. Taiwanese National Health Insurance Dataset. https://dep.mohw.gov.tw/DOS/lp-2506-113.html.
8. Lin LY, Warren-Gash C, Smeeth L. et al. Data resource profile: the National Health Insurance Research Database (NHIRD). Epidemiol Health. 2018;40:e2018062 doi: 10.4178/epih.e2018062
9. Beck M, Ramaswami U, Hernberg-Ståhl E. et al. Twenty years of the Fabry Outcome Survey (FOS): insights, achievements, and lessons learned from a global patient registry. Orphanet J Rare Dis. 2022;17:238 doi: 10.1186/s13023-022-02392-9
10. Burlina AP, Sims KB, Politei JM. et al. Early diagnosis of peripheral nervous system involvement in Fabry disease and treatment of neuropathic pain: the report of an expert panel. BMC Neurol. 2011;11:61 doi: 10.1186/1471-2377-11-61
11. Kokotis P, Zompola C, Anastasakis A. et al. Clinical significance of small nerve fiber involvement in the early diagnosis and treatment of patients with Fabry disease. J Neurol Sci. 2023;453:120776 doi: 10.1016/j.jns.2023.120776
12. Cocozza S, Russo C, Pontillo G. et al. Neuroimaging in Fabry disease: current knowledge and future directions. Insights Imaging. 2018;9:1077-1088 doi: 10.1007/s13244-018-0664-8
13. Albrecht J, Dellani PR, Müller MJ. et al. Voxel based analyses of diffusion tensor imaging in Fabry disease. J Neurol Neurosurg Psychiatry. 2007;78:964-969 doi: 10.1136/jnnp.2006.112987
14. Di Natale D, Rossi S, Dalla Zanna G. et al. Prevalence and Clinical Correlates of Cerebrovascular Alterations in Fabry Disease: A Cross-Sectional Study. Brain Sci. 2025;15:166 doi: 10.3390/brainsci15020166
15. Cocozza S, Schiavi S, Pontillo G. et al. Microstructural damage of the cortico-striatal and thalamo-cortical fibers in Fabry disease: a diffusion MRI tractometry study. Neuroradiology. 2020;62:1459-1466 doi: 10.1007/s00234-020-02497-7
16. Zedde M, Romani I, Scaravilli A. et al. Expanding the Neurological Phenotype of Anderson-Fabry Disease: Proof of Concept for an Extrapyramidal Neurodegenerative Pattern and Comparison with Monogenic Vascular Parkinsonism. Cells. 2024;13:1131 doi: 10.3390/cells13131131
17. Mroczek M, Maniscalco I, Sendel M. et al. Neuropsychiatric Symptoms and Their Association with Sex, Age, and Enzyme Replacement Therapy in Fabry Disease: A Systematic Review. Front Psychiatry. 2022;13:829128 doi: 10.3389/fpsyt.2022.829128
18. Rozenfeld P, Feriozzi S. Contribution of inflammatory pathways to Fabry disease pathogenesis. Mol Genet Metab. 2017;122:19-27 doi: 10.1016/j.ymgme.2017.09.004
19. Faro DC, Di Pino FL, Monte IP. Inflammation, Oxidative Stress, and Endothelial Dysfunction in the Pathogenesis of Vascular Damage: Unraveling Novel Cardiovascular Risk Factors in Fabry Disease. Int J Mol Sci. 2024;25:8273 doi: 10.3390/ijms25158273
20. Hilz M.J, Kolodny E.H, Brys M. et al. Reduced cerebral blood flow velocity and impaired cerebral autoregulation in patients with Fabry disease. J Neurol. 2004 251, 564-570
21. Kolodny E, Fellgiebel A, Hilz MJ. et al. Cerebrovascular involvement in Fabry disease: current status of knowledge. Stroke. 2015;46:302-313 doi: 10.1161/STROKEAHA.114.006283
22. Rolfs A, Böttcher T, Zschiesche M. et al. Prevalence of Fabry disease in patients with cryptogenic stroke: a prospective study. Lancet. 2005;366:1794-1796 doi: 10.1016/S0140-6736(05)67635-0
23. Lee TH, Yang JT, Lee JD. et al. Genomic screening of Fabry disease in young stroke patients: the Taiwan experience and a review of the literature. Eur J Neurol. 2019;26:553-555 doi: 10.1111/ene.13775
24. Levine DA, Galecki AT, Langa KM. et al. Trajectory of Cognitive Decline After Incident Stroke. JAMA. 2015 314, 41-51
25. Plotegher N, Duchen MR. Mitochondrial Dysfunction and Neurodegeneration in Lysosomal Storage Disorders. Trends Mol Med. 2017;23:116-134 doi: 10.1016/j.molmed.2016.12.003
26. Spinelli L, Bianco A, Riccio E. et al. Cardiac involvement in Anderson-Fabry disease. The role of advanced echocardiography. Front Cardiovasc Med. 2024;11:1440636 doi: 10.3389/fcvm.2024.1440636
27. Wilson HC, Hopkin RJ, Madueme PC. et al. Arrhythmia and Clinical Cardiac Findings in Children with Anderson-Fabry Disease. Am J Cardiol. 2017;120:251-255 doi: 10.1016/j.amjcard.2017.04.016
28. Guideline for the prevention of falls in older persons. American Geriatrics Society, British Geriatrics Society, and American Academy of Orthopaedic Surgeons Panel on Falls Prevention. J Am Geriatr Soc. 2001;49:664-672
29. Alosco ML, Penn MS, Spitznagel MB. Reduced physical fitness in patients with heart failure as a possible risk factor for impaired driving performance. Am J Occup Ther. 2015;69:690226001022
30. Falkenstein M, Karthaus M, Brüne-Cohrs U. Age-Related Diseases and Driving Safety. Geriatrics (Basel). 2020;5:80 doi: 10.3390/geriatrics5040080
31. Neto JTD, Kirsztajn GM. The role of podocyte injury in the pathogenesis of Fabry disease nephropathy. J Bras Nefrol. 2024;46:e20240035 doi: 10.1590/2175-8239-JBN-2024-0035en
32. Kleinert J, Dehout F, Schwarting A. et al. Anemia is a new complication in Fabry disease: data from the Fabry Outcome Survey. Kidney Int. 2005;67:1955-60 doi: 10.1111/j.1523-1755.2005.00294.x
33. Cheng YF, Xirasagar S, Chen CS. et al. Association of Fabry Disease with Hearing Loss, Tinnitus, and Sudden Hearing Loss: A Nationwide Population-Based Study. J Clin Med. 2022;11:7396 doi: 10.3390/jcm11247396
34. Page NG, Gresty MA. Motorist's vestibular disorientation syndrome. J Neurol Neurosurg Psychiatry. 1985;48:729-735 doi: 10.1136/jnnp.48.8.729
35. Leng Y, Zhao Y, Zhou H. et al. The vestibular and oculomotor dysfunction in Fabry disease: a cohort study in China. Ann Med. 2025;57:2453626 doi: 10.1080/07853890.2025.2453626
36. Dütsch M, Hilz MJ. Neurological complications in Fabry disease. Rev Med Interne. 2010;31(Suppl2):S243-S250 doi: 10.1016/S0248-8663(10)70021-7
37. Blaszczyk B, Wieckiewicz M, Kusztal M. et al. Fabry disease and sleep disorders: a systematic review. Front Neurol. 2023;14:1217618 doi: 10.3389/fneur.2023.1217618
38. Caputo F, Lungaro L, Galdi A. et al. Gastrointestinal Involvement in Anderson-Fabry Disease: A Narrative Review. Int J Environ Res Public Health. 2021;18:3320 doi: 10.3390/ijerph18063320
39. Bar N, Karaa A, Kiser K. et al. Gastrointestinal Sensory Neuropathy and Dysmotility in Fabry Disease: Presentations and Effect on Patient's Quality of Life. Clin Transl Gastroenterol. 2023;14:e00633 doi: 10.14309/ctg.0000000000000633
40. Cox DJ, Singh H, Lorber D. et al. Diabetes and driving safety: science, ethics, legality and practice. Am J Med Sci. 2013;345:263-265 doi: 10.1097/MAJ.0b013e31828bf8d7
41. Gambardella J, Riccio E, Bianco A. et al. Fatigue as hallmark of Fabry disease: role of bioenergetic alterations. Front Cardiovasc Med. 2024;11:1341590 doi: 10.3389/fcvm.2024.1341590
42. De Marco O, Gambardella J, Bianco A. et al. Cardiopulmonary determinants of reduced exercise tolerance in Fabry disease. Front Cardiovasc Med. 2024;11:1396996 doi: 10.3389/fcvm.2024.1396996
43. Bakar C, Cevizci S, Gündoğar D. et al. Prevalence of unintentional injuries and related risk factors among university students in Canakkale city, western Turkey. Cent Eur J Public Health. 2014;22:189-196 doi: 10.21101/cejph.a3974
44. Wang QR, Lu YY, Su YJ, Wu CH. et al. Migraine and traumatic brain injury: a cohort study in Taiwan. BMJ Open. 2019;9:e027251 doi: 10.1136/bmjopen-2018-027251
45. Diel RJ, Mehra D, Kardon R. et al. Photophobia: shared pathophysiology underlying dry eye disease, migraine and traumatic brain injury leading to central neuroplasticity of the trigeminothalamic pathway. Br J Ophthalmol. 2021;105:751-760 doi: 10.1136/bjophthalmol-2020-316417
46. DiGuiseppi CG, Johnson RL, Betz ME. et al. Migraine headaches are associated with motor vehicle crashes and driving habits among older drivers: Prospective cohort study. J Am Geriatr Soc. 2024;72:791-801 doi: 10.1111/jgs.18719
47. Ito M, Ikaga T, Oguma Y. et al. Association between indoor temperature during winter and falls at home in the past year among community-dwelling older adults: A cross-sectional analysis of the nationwide Smart Wellness Housing survey in Japan. Japanese Journal of Geriatrics. 2024;61:218-227 doi: 10.3143/geriatrics.61.218
48. National Health Insurance Administration, Ministry of Health, Welfare. Indication of Fabry disease. https://www.nhi.gov.tw/ch/np-2505-1.html.
49. Mignani R, Biagini E, Cianci V. et al. Effects of Current Therapies on Disease Progression in Fabry Disease: A Narrative Review for Better Patient Management in Clinical Practice. Adv Ther. 2025;42:597-635 doi: 10.1007/s12325-024-03041-2
50. Baciga F, Marchi G, Caccia F. et al. How Do Physical Activity and Exercise Affect Fabry Disease? Exploring a New Opportunity. Kidney Blood Press Res. 2024;49:699-717 doi: 10.1159/000540236
51. Moore JL, Potter K, Blankshain K. et al. A Core Set of Outcome Measures for Adults with Neurologic Conditions Undergoing Rehabilitation: A CLINICAL PRACTICE GUIDELINE. J Neurol Phys Ther. 2018;42:174-220 doi: 10.1097/NPT.0000000000000229
52. Fritz S, Lusardi M. White paper: “walking speed: the sixth vital sign.”. J Ger Phys Ther. 2009;32:46-49
Author contact
![]() Corresponding author: Chun-An Cheng, Email: ccaedu.tw; Tel.: +886-2-87927173.
Corresponding author: Chun-An Cheng, Email: ccaedu.tw; Tel.: +886-2-87927173.