Impact Factor ISSN: 1449-1907
- Issue 9; 2026
- Issue 8; 2026
- Issue 7; 2026
- Issue 6; 2026
- Issue 5; 2026
- Volume 23; 2026
- Past Issues
- Editorial Board
- Cover Images
- Index & Coverage
- Cover Suggestion
- Special Issues
Introduction
Materials and Methods
Results
Discussion
Conclusion
Abbreviations
Acknowledgements
References

 Global reach, higher impact
Global reach, higher impactInt J Med Sci 2026; 23(7):2277-2289. doi:10.7150/ijms.131653 This issue Cite
Research Paper
Expanding Outcomes Beyond Chronic Kidney Disease-Mineral and Bone Disorder: A Propensity Score-Matched Analysis of Parathyroidectomy versus Calcimimetics in Dialysis Patients with Secondary Hyperparathyroidism
Yi-Chou Hou1, Cai-Mei Zheng2,3,4, Ko-Lin Kuo5,6,7, Kuo-Wang Tsai8,9, Joshua Wang8, Cheng-Yi Wang10, Ruei-Ming Chen11,12,13, Kuo-Cheng Lu5,14 ![]()
1. Division of Nephrology, Department of Internal Medicine, Cardinal Tien Hospital, School of Medicine, Fu Jen Catholic University, New Taipei City, Taiwan.
2. Division of Nephrology, Department of Internal Medicine, Shuang Ho Hospital, Taipei Medical University, New Taipei City, Taiwan.
3. Division of Nephrology, Department of Internal Medicine, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan.
4. TMU Research Centre of Urology and Kidney, Taipei Medical University, Taipei, Taiwan.
5. Division of Nephrology, Department of Medicine, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City, Taiwan.
6. School of Medicine, Tzu Chi University, Hualien, Taiwan.
7. School of Post-Baccalaureate Chinese Medicine, Tzu Chi University, Hualien, Taiwan.
8. Department of Research, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, New Taipei City 23142, Taiwan.
9. Department of Nursing, Cardinal Tien Junior College of Healthcare and Management, New Taipei City 23143, Taiwan.
10. Division of Pulmonology, Department of Internal Medicine, Cardinal Tien Hospital, School of Medicine, Fu Jen Catholic University, New Taipei City, Taiwan.
11. Cell Physiology and Molecular Image Research Center, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan.
12. Graduate Institute of Medical Sciences, College of Medicine, Taipei Medical University, Taipei, Taiwan.
13. Anesthesiology and Health Policy Research Center, Taipei Medical University Hospital, Taipei, Taiwan.
14. Division of Nephrology, Department of Medicine, Fu Jen Catholic University Hospital, School of Medicine, Fu Jen Catholic University, New Taipei City, Taiwan.
Received 2026-1-17; Accepted 2026-5-5; Published 2026-5-22
Abstract

Background: Secondary hyperparathyroidism (SHPT) is a common complication in patients with end-stage renal disease (ESRD) receiving dialysis. Although calcimimetics (CAMs) and parathyroidectomy (PTx) are widely used for severe SHPT, their comparative effects on long-term clinical outcomes beyond mineral and bone disorder remain uncertain.
Methods: We conducted a retrospective multicenter cohort study using the TriNetX research network (2010-2024). Adult dialysis patients with ESRD and severe SHPT, defined by at least one historical intact parathyroid hormone level >600 pg/mL prior to treatment initiation, were included. Patients receiving both therapies were excluded. After 1:1 propensity score matching for demographics, comorbidities, medications, and laboratory variables, outcomes including all-cause mortality, major adverse cardiovascular events (MACE), fracture, cognitive impairment, mild cognitive impairment (MCI), and sepsis were compared using Cox proportional hazards models.
Results: After propensity score matching, 22,580 patients were included (11,290 in each group), with follow-up extending to 7 years. Compared with CAM therapy, PTx was associated with significantly lower risks of all-cause mortality (hazard ratio [HR] 0.914, 95% confidence interval [CI] 0.860-0.972), mild cognitive impairment (HR 0.646, 95% CI 0.436-0.955), and sepsis (HR 0.844, 95% CI 0.765-0.930). No significant differences were observed for MACE, fracture, hungry bone disease, overall cognitive impairment, or malignancy.
Conclusion: In patients with ESRD and severe SHPT, parathyroidectomy was associated with lower risks of mortality, mild cognitive impairment, and sepsis compared with calcimimetic therapy, while cardiovascular and fracture outcomes were comparable. These findings suggest that PTx may confer broader systemic benefits beyond mineral and bone disorder control in selected dialysis patients.
Keywords: end-stage renal disease, secondary hyperparathyroidism, parathyroidectomy, calcimimetics, mortality, cognitive impairment, sepsis
Introduction
Secondary hyperparathyroidism (SHPT) represents a frequent and debilitating complication in patients with end-stage renal disease (ESRD) undergoing dialysis. SHPT results from the interplay of phosphate retention, hypocalcemia, and reduced vitamin D activation, leading to chronic stimulation of the parathyroid glands [1, 2]. Sustained hyperparathyroidism causes metabolic bone disorder, vascular calcification, anemia, and systemic inflammation. Elevated parathyroid hormone (PTH) levels are not only markers of mineral imbalance but also correlate with higher mortality, hospitalization, and impaired quality of life [3].
Therapeutic approaches for SHPT include pharmacological treatment with calcimimetics (CAMs) and surgical parathyroidectomy (PTx). CAMs such as cinacalcet and etelcalcetide allosterically activate the calcium-sensing receptor to reduce PTH secretion [4, 5]. They have demonstrated efficacy in lowering serum PTH, calcium, and phosphorus. However, their long-term impact on hard clinical outcomes remains controversial, as randomized controlled trials (RCTs) have yielded mixed results [6, 7]. PTx, by contrast, directly removes hyperplastic parathyroid glands, leading to sustained biochemical control and often greater improvements in calcium-phosphate homeostasis.
Despite these mechanistic differences, evidence comparing PTx and CAMs in real-world populations remains limited. Most prior studies have focused on mortality or cardiovascular outcomes, while neglecting broader systemic complications of ESRD [7, 8]. Two outcomes of particular relevance are cognitive impairment and infection risk. Cognitive impairment is highly prevalent among dialysis patients, with estimates ranging from 30% to 60% [9, 10]. It arises from a combination of uremic toxin accumulation, cerebral microvascular disease, oxidative stress, and chronic inflammation. Similarly, sepsis is one of the leading causes of death and hospitalization in dialysis patients, reflecting impaired immune function and frequent vascular access exposure [11]. Whether improved biochemical control from PTx translates into reduced neurocognitive decline or lower sepsis burden has not been systematically studied.
The present study therefore addresses this critical gap. Using a large federated network of electronic health records, we compared the long-term outcomes of ESRD patients with severe SHPT treated with PTx versus CAMs. We hypothesized that, beyond survival, PTx would confer systemic benefits, including reduced risk of cognitive impairment and sepsis, compared with CAM therapy.
Materials and Methods
Study Design and Data SourceThis was a retrospective multicenter cohort study conducted using the TriNetX research network, which integrates de-identified electronic medical records (EMRs) from 84 healthcare organizations. The database includes demographic characteristics, diagnoses, procedures, medications, laboratory values, and longitudinal outcomes. The study period spanned from January 1, 2010, to June 30, 2024, with a maximum follow-up duration of 7 years.
Study Population and Index Date
This retrospective cohort study was conducted using the TriNetX research network. Eligible patients were adults with end-stage renal disease (ESRD) who subsequently developed severe secondary hyperparathyroidism (SHPT), defined as the presence of at least one documented intact parathyroid hormone (iPTH) measurement exceeding 600 pg/mL. ESRD was identified by the ICD-10-CM diagnosis code N18.6 for 3 times.
Patients were classified into two mutually exclusive treatment groups:
- Parathyroidectomy (PTx) cohort: Patients who had undergone parathyroidectomy after initiating dialysis. PTx was identified by ICD-10-PCS and CPT procedure codes, including excision, resection, destruction, subtotal, or total parathyroidectomy procedures. The index date was defined as the date of the first qualifying parathyroidectomy (Table 1).
- Calcimimetic (CAMs) cohort: Patients who received calcimimetic therapy (cinacalcet, etelcalcetide, or evocalcet; coding definitions are listed in Table 1) after dialysis initiation, with iPTH >600 pg/mL at baseline. The index date was defined as the date of the first prescription of a calcimimetic agent.
Coding of clinical indicators of the study
| Death |
|---|
| Demographics: Deceased |
| Fracture (ICD-10-CM codes) |
| S12: Cervical vertebra / neck S22: Rib, sternum, thoracic spine S32: Lumbar spine, pelvis S42: Shoulder, upper arm S52: Forearm S62: Wrist, hand S72: Femur S82: Lower leg, ankle S92: Foot, toe |
| Major Adverse Cardiovascular Events (MACE) (ICD-10-CM codes) |
| I20-I25: Ischemic heart diseases I63: Cerebral infarction I50: Heart failure I70-I79: Peripheral arterial disease I49: Other cardiac arrhythmias |
| Hungry Bone Syndrome |
| E83.81: Hungry bone syndrome M89.30: Hypertrophy of bone, unspecified site |
| Cognitive Impairment / Dementia (ICD-10-CM codes) |
| F03: Unspecified dementia F02: Dementia in other diseases classified elsewhere F01: Vascular dementia G30: Alzheimer's disease |
| Mild Cognitive Impairment (MCI) |
| G31.84: Mild cognitive impairment of uncertain or unknown etiology |
| Parathyroid Hormone (PTH) |
| LOINC 2731-8: Parathyrin, intact [Mass/volume] in Serum or Plasma |
| Malignancies (exploratory outcome) (ICD-10-CM codes) |
| C00-C14: Lip, oral cavity, pharynx C15-C26: Digestive organs C30-C39: Respiratory / intrathoracic organs C50: Breast C64-C68: Urinary tract |
| Calcimimetics (CAMs) |
| RxNorm 407990: Cinacalcet RxNorm 1876119: Etelcalcetide HCPCS J0604: Cinacalcet, oral, 1 mg (ESRD on dialysis) |
| Parathyroidectomy (PTx) |
| ICD-10-PCS: 0GBR0ZZ, 0GBR3ZZ, 0GBR4ZZ (Excision) ICD-10-PCS: 0GTR0ZZ, 0GTR4ZZ (Resection) ICD-10-PCS: 0G5R0ZZ, 0G5R3ZZ, 0G5R4ZZ (Destruction) SNOMED: 53304009, 12330002, 63382008, 171995003, 171997006, 41237009 CPT: 60500, 60502, 60505, 1014226 ICD-10-CM: Z98.89 (Other postprocedural states), Z90.89 (Acquired absence of other organs) |
| Dialysis |
| CPT: 1012740 (Dialysis services and procedures) CPT: 90945 (Dialysis, non-hemodialysis, peritoneal, hemofiltration, CRRT) CPT: 1012757 (Miscellaneous dialysis services) ICD-9-CM: 39.95 (Hemodialysis) ESRD-related service codes: monthly (2-3 visits / ≥4 visits), per-day service for patients >20 years |
Patients were excluded if they received both PTx and CAM therapy, either before the index date or within ±90 days of each other, to ensure mutually exclusive exposure groups. Patients with iPTH ≤600 pg/mL prior to treatment, those with acute kidney injury (AKI), or those lacking complete demographic or follow-up information were also excluded.
The analysis time window was defined from 365 days after the index event to 2555 days (7 years) after the index event. This approach minimized immortal time bias by excluding outcomes within the first year after treatment initiation and ensured sufficient follow-up for long-term outcomes. Patients whose index event occurred more than 20 years prior to the analysis date were excluded, although no such cases were identified in this study.
Exposures and Outcomes
The primary and secondary study outcomes were defined using standardized ICD-10-CM codes listed as Table 1. All-cause mortality was determined based on death status recorded in the electronic health record. Major adverse cardiovascular events (MACE) were defined as a composite of ischemic heart diseases (I20-I25), cerebral infarction (I63), heart failure (I50), diseases of arteries, arterioles, and capillaries (I70-I79), and other cardiac arrhythmias (I49). Fracture events were identified using diagnostic codes for fractures of the cervical spine and neck (S12), thoracic spine and rib cage (S22), lumbar spine and pelvis (S32), shoulder and upper arm (S42), forearm (S52), wrist and hand (S62), femur (S72), lower leg including ankle (S82), and foot or toe excluding ankle (S92). Hungry bone syndrome was defined by either the presence of a diagnosis code for hungry bone syndrome (E83.81) or hypertrophy of bone of unspecified site (M89.30).
Neurocognitive outcomes were also included. Cognitive impairment and dementia encompassed unspecified dementia (F03), dementia in other diseases classified elsewhere (F02), Alzheimer's disease (G30), and vascular dementia (F01). In addition, mild cognitive impairment (MCI) was defined as the presence of a diagnosis code for mild cognitive impairment of uncertain or unknown etiology (G31.84). Malignancy was defined by incident diagnoses of malignant neoplasms involving the lip, oral cavity, and pharynx (C00-C14); digestive organs (C15-C26); respiratory and intrathoracic organs (C30-C39); breast (C50); and urinary tract (C64-C68). Finally, sepsis was defined as a diagnosis of sepsis (A41).
Covariates
Baseline variables included demographics (age, sex, race/ethnicity), comorbidities (diabetes mellitus, hypertension, ischemic heart disease, heart failure, cerebrovascular disease, peripheral vascular disease, chronic obstructive pulmonary disease, chronic liver disease, malignancy), and dialysis vintage. Laboratory data, when available, included hemoglobin, serum calcium, phosphate, and estimated glomerular filtration rate (eGFR).
Statistical Analysis
Propensity score matching was conducted on 32 baseline characteristics, including demographics (age, sex, race, ethnicity), comorbidities (hypertension, ischemic heart disease, cerebrovascular disease, diabetes, and other cardiovascular conditions), medication use (ACE inhibitors, angiotensin II inhibitors, vitamin D, calcium channel blockers, bisphosphonates, calcium, GLP-1 analogues, DPP-4 inhibitors, and other bone/mineralization agents), and laboratory parameters (intact parathyroid hormone, serum calcium, hemoglobin, and calcidiol). Cohorts were balanced 1:1 using these covariates, and the baseline characteristics before and after matching are summarized in Table 2. Kaplan-Meier survival curves were generated, and hazard ratios (HRs) with 95% confidence intervals (CIs) were estimated using Cox proportional hazards models. Subgroup analyses were performed to explore whether the association between treatment strategy and outcomes varied across predefined clinical and biochemical strata. Hazard ratios were calculated by comparing patients with versus without each specified factor. These analyses were intended to assess effect modification rather than to determine independent causal effects of individual variables. A two-sided p-value < 0.05 was considered statistically significant.
Demographic and baseline characteristics between PTx CAMS groups
| Parameter | PTx (n=14,281) | CAMs (n=19,311) | P value | Std Diff | PTx (n=11,290) | CAMs (n=11,290) | P value | Std Diff |
|---|---|---|---|---|---|---|---|---|
| Demographics | ||||||||
| Age at index, mean ± SD | 60.8 ± 15.1 | 57.6 ± 15.2 | <0.001 | 0.212 | 59.6 ± 15.6 | 59.4 ± 14.4 | 0.406 | 0.011 |
| Female, n (%) | 6,188 (42.7) | 8,578 (44.6) | <0.001 | 0.039 | 4,936 (43.7) | 4,963 (44.0) | 0.717 | 0.005 |
| Male, n (%) | 8,224 (56.7) | 10,556 (54.9) | 0.001 | 0.037 | 6,291 (55.7) | 6,265 (55.5) | 0.728 | 0.005 |
| White, n (%) | 7,476 (51.6) | 6,580 (34.2) | <0.001 | 0.356 | 4,912 (43.5) | 4,945 (43.8) | 0.658 | 0.006 |
| Black or African American, n (%) | 4,946 (34.1) | 8,533 (44.4) | <0.001 | 0.211 | 4,475 (39.6) | 4,468 (39.6) | 0.924 | 0.001 |
| Asian, n (%) | 726 (5.0) | 1,083 (5.6) | 0.012 | 0.028 | 628 (5.6) | 647 (5.7) | 0.584 | 0.007 |
| Hispanic or Latino, n (%) | 2,599 (17.9) | 2,221 (11.6) | <0.001 | 0.181 | 1,570 (13.9) | 1,568 (13.9) | 0.969 | 0.001 |
| Underlying illness | ||||||||
| Hypertensive diseases, n (%) | 13,763 (94.9) | 17,001 (88.4) | <0.001 | 0.237 | 10,579 (93.7) | 10,623 (94.1) | 0.221 | 0.016 |
| Ischemic heart disease, n (%) | 8,272 (57.1) | 8,378 (43.6) | <0.001 | 0.272 | 5,899 (52.2) | 5,935 (52.6) | 0.631 | 0.006 |
| Other heart disease, n (%) | 11,256 (77.6) | 12,505 (65.0) | <0.001 | 0.281 | 8,403 (74.4) | 8,473 (75.0) | 0.284 | 0.014 |
| Cerebrovascular disease, n (%) | 3,643 (25.1) | 3,305 (17.2) | <0.001 | 0.195 | 2,465 (21.8) | 2,478 (21.9) | 0.834 | 0.003 |
| Diseases of arteries/arterioles, n (%) | 6,845 (47.2) | 6,275 (32.6) | <0.001 | 0.301 | 4,691 (41.6) | 4,689 (41.5) | 0.978 | <0.001 |
| Diabetes mellitus, n (%) | 10,080 (69.5) | 10,219 (53.2) | <0.001 | 0.341 | 7,213 (63.9) | 7,261 (64.3) | 0.505 | 0.009 |
| Medications | ||||||||
| Beta blockers, n (%) | 11,353 (78.3) | 14,134 (73.5) | <0.001 | 0.112 | 8,640 (76.5) | 8,635 (76.5) | 0.937 | 0.001 |
| Antilipemic agents, n (%) | 8,961 (61.8) | 10,592 (55.1) | <0.001 | 0.137 | 6,572 (58.2) | 6,925 (61.3) | <0.001 | 0.064 |
| Antihypertensives, other, n (%) | 8,723 (60.2) | 9,748 (50.7) | <0.001 | 0.191 | 6,582 (58.3) | 5,961 (52.8) | <0.001 | 0.111 |
| ACE inhibitors, n (%) | 3,150 (21.7) | 4,837 (25.2) | <0.001 | 0.081 | 2,587 (22.9) | 2,609 (23.1) | 0.728 | 0.005 |
| Angiotensin II inhibitors, n (%) | 3,646 (25.2) | 4,367 (22.7) | <0.001 | 0.057 | 2,763 (24.5) | 2,685 (23.8) | 0.225 | 0.016 |
| Calcium channel blockers, n (%) | 8,532 (58.9) | 11,098 (57.7) | 0.037 | 0.023 | 6,599 (58.4) | 6,569 (58.2) | 0.686 | 0.005 |
| Insulin, n (%) | 9,557 (65.9) | 10,294 (53.5) | <0.001 | 0.255 | 6,917 (61.3) | 6,891 (61.0) | 0.723 | 0.005 |
| Vitamin D, n (%) | 7,051 (48.6) | 9,421 (49.0) | 0.508 | 0.007 | 5,465 (48.4) | 5,488 (48.6) | 0.759 | 0.004 |
| Bisphosphonates, n (%) | 100 (0.7) | 114 (0.6) | 0.268 | 0.012 | 75 (0.7) | 75 (0.7) | 1.000 | <0.001 |
| GLP-1 analogues, n (%) | 393 (2.7) | 304 (1.6) | <0.001 | 0.078 | 240 (2.1) | 242 (2.1) | 0.927 | 0.001 |
| DPP-4 inhibitors, n (%) | 659 (4.5) | 523 (2.7) | <0.001 | 0.098 | 401 (3.6) | 404 (3.6) | 0.914 | 0.001 |
| Calcium, n (%) | 8,711 (60.1) | 8,875 (46.2) | <0.001 | 0.282 |
Results
Study Population
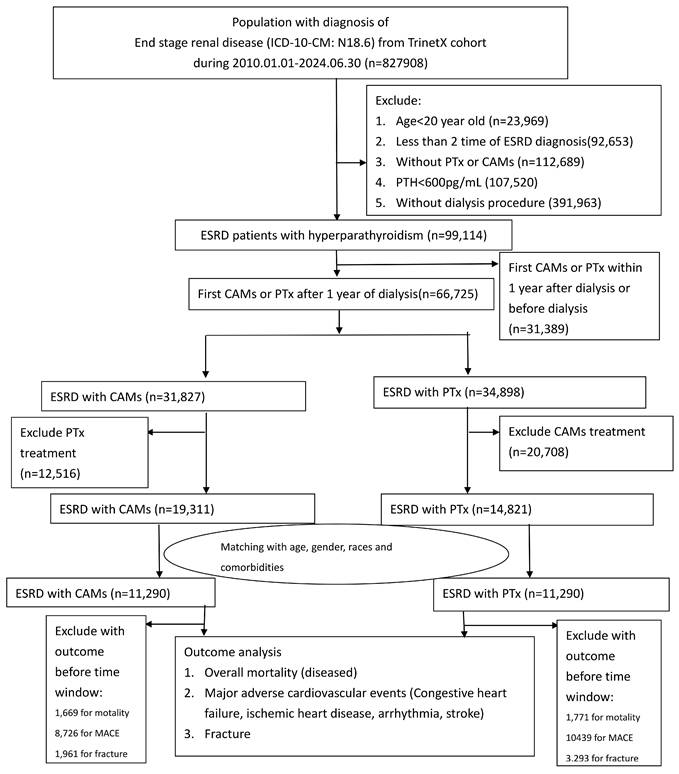
Figure 1 illustrated the flow chart of the study. A total of 34,133 patients with ESRD and severe SHPT (PTH > 600 pg/mL) were identified. After 1:1 propensity score matching, 22,580 patients remained in the analytic cohort, comprising 11,290 who underwent PTx and 11,290 treated with CAM therapy.
Flow chart of patient selection. Patients with end-stage renal disease (ESRD; ICD-10-CM: N18.6) were identified from the TriNetX research network (2010-2024). After applying sequential exclusions for age <20 years, insufficient ESRD diagnoses, absence of dialysis procedures, parathyroid hormone (PTH) <600 pg/mL, early treatment exposure, and prior outcomes, 11,290 patients undergoing parathyroidectomy (PTx) and 11,290 patients receiving calcimimetics (CAMs) were included following 1:1 propensity score matching for demographics, comorbidities, laboratory data, and medication use.
Before matching, the PTx and CAMs groups differed significantly in demographic, diagnostic, and medication profiles. After 1:1 propensity score matching, baseline characteristics were well balanced: age, sex, race, and ethnicity were comparable between groups; the prevalence of major comorbidities, including hypertension, diabetes, ischemic heart disease, and cerebrovascular disease, was similar; and the distribution of medication use (ACE inhibitors, angiotensin II inhibitors, vitamin D, calcium channel blockers, bisphosphonates, calcium, GLP-1 analogues, and DPP-4 inhibitors) was nearly identical. All standardized differences were reduced to < 0.1, confirming adequate covariate balance across matched cohorts (Table 2). The laboratory results were listed as Table 3.
Laboratory data between PTx CAMS groups
| Parameter | PTx (n, %) | CAMs (n, %) | P value | Std Diff | PTx (n, %) | CAMs (n, %) | P value | Std Diff |
|---|---|---|---|---|---|---|---|---|
| Before PSM | After PSM | |||||||
| Phosphate (mg/dL) | 4.6 ± 1.7 | 5.2 ± 1.9 | < 0.001 | 0.307 | 4.7 ± 1.7 | 5.1 ± 1.8 | < 0.001 | 0.237 |
| 3.5-5.5 mg/dL | 8,873 (61.2) | 10,638 (55.3) | < 0.001 | 0.119 | 6,668 (59.1) | 6,557 (58.1) | 0.134 | 0.020 |
| 5.5-6.5 mg/dL | 5,886 (40.6) | 7,912 (41.2) | 0.308 | 0.011 | 4,405 (39.0) | 4,783 (42.4) | < 0.001 | 0.068 |
| 6.5-7.5 mg/dL | 4,027 (27.8) | 5,964 (31.0) | < 0.001 | 0.071 | 3,025 (26.8) | 3,558 (31.5) | < 0.001 | 0.104 |
| 2.5-3.5 mg/dL | 5,811 (40.1) | 5,751 (29.9) | < 0.001 | 0.214 | 4,254 (37.7) | 3,692 (32.7) | < 0.001 | 0.104 |
| Calcium (mg/dL) | 8.8 ± 0.8 | 9.0 ± 0.9 | < 0.001 | 0.208 | 8.8 ± 0.8 | 8.9 ± 0.9 | < 0.001 | 0.069 |
| 8.5-10.5 mg/dL | 11,682 (80.6) | 14,992 (78.0) | < 0.001 | 0.064 | 8,936 (79.1) | 8,889 (78.7) | 0.443 | 0.010 |
| 10.5-12 mg/dL | 1,590 (11.0) | 2,980 (15.5) | < 0.001 | 0.134 | 1,392 (12.3) | 1,437 (12.7) | 0.366 | 0.012 |
| 12-14 mg/dL | 141 (1.0) | 224 (1.2) | 0.091 | 0.019 | 111 (1.0) | 125 (1.1) | 0.360 | 0.012 |
| 7-8.5 mg/dL | 9,085 | 9,719 | < 0.001 | 0.246 | 6,513 | 6,533 | 0.788 | 0.004 |
| Creatinine (mg/dL) | 6.1 ± 3.2 | 7.9 ± 4.0 | < 0.001 | 0.495 | 6.3 ± 3.3 | 7.6 ± 3.6 | < 0.001 | 0.366 |
| Hemoglobin (g/dL) | 10.0 ± 1.9 | 10.3 ± 1.9 | < 0.001 | 0.125 | 10.1 ± 2.0 | 10.2 ± 1.9 | < 0.001 | 0.095 |
| 9-10 g/dL | 9,212 (63.5) | 10,397 (54.1) | < 0.001 | 0.193 | 6,704 (59.4) | 6,710 (59.4) | 0.935 | 0.001 |
| 10-11 g/dL | 9,388 (64.8) | 11,071 (57.6) | < 0.001 | 0.148 | 6,957 (61.6) | 6,938 (61.5) | 0.795 | 0.003 |
| 11-12 g/dL | 8,359 (57.7) | 9,969 (51.9) | < 0.001 | 0.117 | 6,192 (54.8) | 6,213 (55.0) | 0.779 | 0.004 |
| >12 g/dL | 6,436 (44.4) | 7,796 (40.5) | < 0.001 | 0.078 | 4,818 (42.7) | 4,817 (42.7) | 0.989 | < 0.001 |
| Other labs | ||||||||
| Platelets (×10⁹/L) | 205.1 ± 91.3 (12,552; 86.6) | 203.1 ± 83.2 (16,539; 86.0) | 0.050 | 0.023 | 205.3 ± 90.3 (9,594; 85.0) | 201.3 ± 83.3 (9,931; 88.0) | 0.002 | 0.045 |
| Alkaline phosphatase (U/L) | 121.8 ± 94.6 | 134.7 ± 114.1 | < 0.001 | 0.123 | 121.5 ± 97.5 | 131.9 ± 98.6 | < 0.001 | 0.106 |
| Albumin (g/dL) | 3.3 ± 0.7 | 3.5 ± 0.7 | < 0.001 | 0.309 | 3.3 ± 0.7 | 3.5 ± 0.7 | < 0.001 | 0.202 |
| 3.5-4.0 g/dL | 7,752 (53.5) | 9,796 (51.0) | < 0.001 | 0.050 | 5,797 (51.3) | 5,962 (52.8) | 0.028 | 0.029 |
| 4.0-4.5 g/dL | 5,074 (35.0) | 7,133 (37.1) | < 0.001 | 0.044 | 3,876 (34.3) | 4,175 (37.0) | < 0.001 | 0.055 |
| Cholesterol (mg/dL) | 141.7 ± 47.6 | 149.1 ± 47.9 | < 0.001 | 0.156 | 144.2 ± 47.8 | 145.8 ± 47.6 | 0.124 | 0.033 |
| LDL cholesterol (mg/dL) | 72.6 ± 36.9 | 77.0 ± 37.1 | < 0.001 | 0.118 | 74.4 ± 37.1 | 74.6 ± 36.9 | 0.785 | 0.006 |
| HDL cholesterol (mg/dL) | 42.5 ± 17.8 | 43.7 ± 17.1 | < 0.001 | 0.069 | 43.3 ± 18.2 | 43.1 ± 17.0 | 0.570 | 0.012 |
| BNP (pg/mL) | 1,670.4 ± 4,096.1 (4,178; 28.8) | 2,065.4 ± 7,829.1 (4,261; 22.2) | 0.004 | 0.063 | 1,570.4 ± 3,769.9 (3,021; 26.8) | 2,168.6 ± 7,385.7 (2,791; 24.7) | < 0.001 | 0.102 |
| HbA1c (%) | 6.4 ± 1.7 | 6.2 ± 1.7 | < 0.001 | 0.136 | 6.4 ± 1.7 | 6.3 ± 1.7 | 0.007 | 0.050 |
| LVEF (%) | 52.9 ± 14.6 | 54.1 ± 14.3 | 0.023 | 0.079 | 53.1 ± 14.7 | 53.2 ± 14.6 | 0.860 | 0.007 |
| 25(OH)D (ng/mL) | 27.9 ± 17.4 | 26.0 ± 16.4 | 0.001 | 0.113 | 27.3 ± 16.9 | 26.7 ± 16.5 | 0.348 | 0.039 |
The Comparison between CAMs and PTx
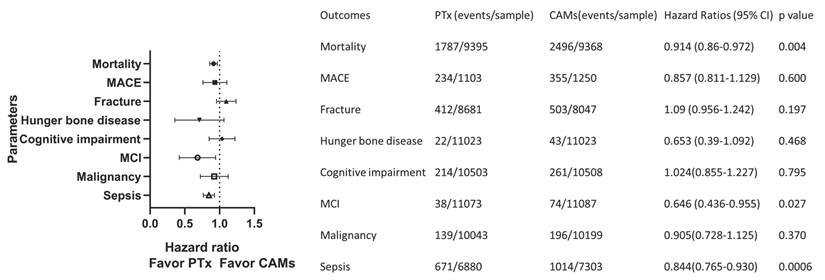
Figure 2 shows the hazard ratios for major outcomes after propensity score matching. Compared with CAM therapy, PTx was associated with significantly lower risks of all-cause mortality (HR 0.914, 95% CI 0.860-0.972, p = 0.004), mild cognitive impairment (HR 0.646, 95% CI 0.436-0.955, p = 0.027), and sepsis (HR 0.844, 95% CI 0.765-0.930, p = 0.0006). No significant differences were observed for MACE, fracture, hungry bone disease, overall cognitive impairment, or malignancy.
Forest plot of major outcomes comparing PTx and CAMs after propensity score matching. PTx was associated with lower risks of all-cause mortality (HR 0.914, 95% CI 0.860-0.972), mild cognitive impairment (HR 0.646, 95% CI 0.436-0.955), and sepsis (HR 0.844, 95% CI 0.765-0.930). No significant differences were observed for MACE, fracture, hungry bone disease, overall cognitive impairment, or malignancy.
All-cause Mortality
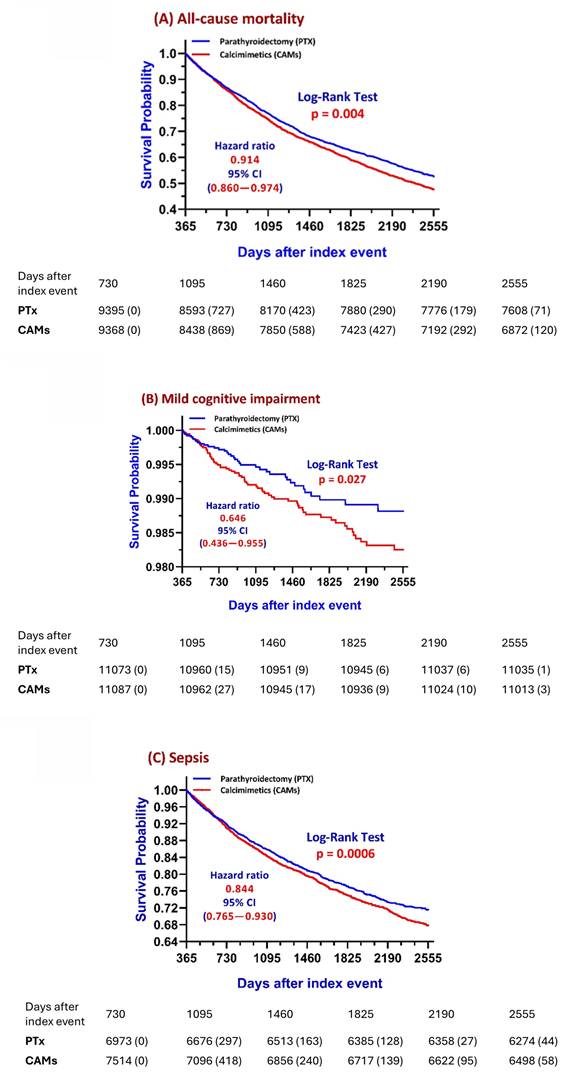
PTx was associated with a significantly lower risk of all-cause mortality compared with CAM therapy. Kaplan-Meier curves showed early separation after the first year and persistent divergence throughout follow-up (Figure 3A). In Cox proportional hazards analysis, PTx was associated with an 8.6% lower mortality risk (HR 0.914, 95% CI 0.860-0.972, p = 0.004). Figure 4A illustrated the subgroup analysis among the subjects receiving PTx. Patients with adequate nutritional and hematologic profiles, particularly those with higher hemoglobin (> 9 g/dL) experienced significantly lower mortality risk, highlighting the protective effect of preserved nutritional status. Conversely, disturbances in mineral metabolism, such as hyperphosphatemia (> 6.0 mg/dL) or hypoalbuminemia was associated with greater risk, though the overall survival benefit of PTx remained consistent. Medication-related subgroups revealed modest risk increases among non-calcium phosphate binders (HR: 1.252, 95%CI:1.139-1.376, p < 0.05), whereas exposure to GLP1-RA had a protective impact (HR: 0.506, 95%CI:0.357-0.718, p < 0.05) (Figure 4A). To assess the robustness of the primary survival findings, additional landmark sensitivity analyses were performed using propensity score-matched cohorts with follow-up windows starting at 90 days and 180 days after the index date. Minor variations in cohort counts were observed across repeated analyses because TriNetX returns data dynamically according to contributing healthcare organizations at the time of query execution. In the 90-2100 day analysis, which included 760 patients in the PTx group and 28,372 in the CAMs group, PTx was associated with significantly lower mortality than CAMs (HR 0.451, 95% CI 0.357-0.570; log-rank P < 0.0001). Similar findings were observed in the 180-2100 day analysis, which included 754 patients in the PTx group and 28,492 in the CAMs group (HR 0.447, 95% CI 0.321-0.623; P = 0.0021).
Kaplan-Meier survival curves for major outcomes after propensity score matching. (A) All-cause mortality: PTx was associated with lower mortality risk compared with CAMs (HR 0.91, 95% CI 0.86-0.97, p = 0.004). (B) Mild cognitive impairment (MCI): PTx was associated with lower incidence of MCI (HR 0.65, 95% CI 0.44-0.96, p = 0.027). (C) Sepsis: PTx was associated with lower sepsis risk compared with CAMs (HR 0.84, 95% CI 0.77-0.93, p < 0.001). Numbers at risk are shown below each panel. Group comparisons were assessed using log-rank tests; hazard ratios were estimated using Cox proportional hazards models.
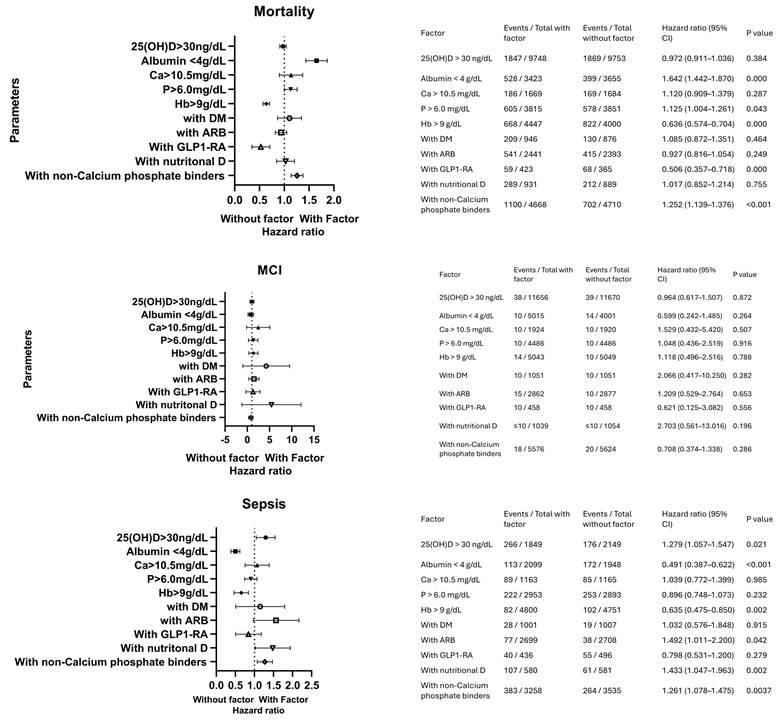
Subgroup analyses of treatment effects comparing PTx and CAMs. Forest plots show hazard ratios with 95% confidence intervals for prespecified clinical and biochemical subgroups. (A) Mortality: the association between PTx and lower mortality was generally consistent across subgroups; stronger associations were observed in patients with hemoglobin >9 g/dL, whereas higher risk was noted in those with low albumin (<4 g/dL), phosphorus >6.0 mg/dL, nutritional vitamin D use, and non-calcium phosphate binder therapy. (B) Mild cognitive impairment (MCI): no significant interaction was observed across subgroups. (C) Sepsis: PTx was associated with lower sepsis risk across most subgroups, whereas higher 25(OH)D levels, ARB use, nutritional vitamin D, and non-calcium phosphate binder therapy were associated with higher relative risk. Hazard ratios were estimated using Cox proportional hazards models.
Outcomes Related to CKD-MBD (Fracture and Cardiovascular Events)
With respect to CKD-MBD-related outcomes, fracture risk did not significantly differ between groups (HR 1.090, 95% CI 0.956-1.242, p = 0.197). Likewise, no significant difference was observed for MACE (HR 0.857, 95% CI 0.811-1.129, p = 0.600) or hungry bone disease (HR 0.653, 95% CI 0.390-1.092, p = 0.468).
Cognitive Impairment
No significant difference was observed in overall cognitive impairment between groups (HR 1.024, 95% CI 0.855-1.227, p = 0.795). However, PTx was associated with a significantly lower risk of mild cognitive impairment (MCI) compared with CAM therapy (HR 0.646, 95% CI 0.436-0.955, p = 0.027) (Figure 3B). Subgroup analysis did not identify any significant modifier of MCI risk, with all confidence intervals crossing unity (Figure 4B).
Sepsis
PTx was also associated with a reduced risk of sepsis (HR 0.76, 95% CI 0.63-0.91, p = 0.004) (Figure 3C). In subgroup analyses, serum albumin level, hemoglobin level, nutritional vitamin D use, non-calcium phosphate binder therapy, and 25(OH)D status demonstrated significant associations with sepsis risk. Other factors, including calcium, phosphorus, diabetes, and newer antidiabetic agents, were not significantly associated with sepsis risk (Figure 4C).
Discussion
In this large multicenter real-world cohort of patients with ESRD and severe SHPT, PTx was associated with significantly lower risks of all-cause mortality, mild cognitive impairment, and sepsis compared with CAM therapy. In contrast, fracture, MACE, hungry bone disease, overall cognitive impairment, and malignancy were comparable between groups.
Mortality Benefit
The most consistent finding was the lower long-term mortality associated with PTx. Although the effect size was modest, survival curves showed early and persistent separation favoring surgery. This benefit may relate to durable PTH control, reduced calcium-phosphate burden, and mitigation of chronic inflammation. Residual mortality risk remained higher among patients with hypoalbuminemia, hyperphosphatemia, and those requiring non-calcium phosphate binders, indicating that malnutrition and severe mineral dysregulation continue to influence prognosis even after surgery. The consistency of mortality reduction across alternative landmark windows (90 and 180 days) further supports that the observed survival benefit of PTx was robust and unlikely to be explained solely by survivor bias related to delayed follow-up initiation. Previous studies have consistently demonstrated that parathyroidectomy (PTx) confers a survival advantage compared with standard care in patients with severe SHPT. A meta-analysis by Song et al. reported an association between PTx and improved survival [12], and similar findings have been observed in large real-world cohorts, including the Japanese dialysis registry [5]. Calcimimetics (CAMs), on the other hand, effectively reduce parathyroid hormone levels through activation of the calcium-sensing receptor and may improve biochemical control without increasing calcium load, thereby potentially mitigating vascular calcification compared with active vitamin D therapy [13, 14]. However, evidence regarding their impact on hard clinical outcomes remains heterogeneous. While individual agents such as etelcalcetide have demonstrated efficacy in PTH suppression and have shown favorable effects on surrogate markers—including modulation of calcium balance [15] , reduction in fibroblast growth factor 23 and attenuation of left ventricular hypertrophy [16] , and improvement in serum calcification propensity (T₅₀)[17]—these findings are primarily mechanistic or intermediate outcomes rather than definitive clinical endpoints. In contrast, comparative observational data suggest that PTx may provide more durable survival benefits than calcimimetic therapy in patients with advanced SHPT [7]. The sustained and profound reduction in PTH achieved with surgery may contribute to improved outcomes through reduction of mineral imbalance, vascular calcification, and systemic inflammation. In our cohort, the mortality benefit associated with PTx remained evident across analyses, although its magnitude appeared influenced by underlying patient characteristics.
Subgroup analyses further highlighted the importance of nutritional and metabolic status. Patients with hypoalbuminemia exhibited less favorable outcomes, consistent with the established role of the malnutrition-inflammation complex in dialysis populations [18,19]. Additionally, the observed associations between higher mortality risk and the use of non-calcium phosphate binders, angiotensin receptor blockers, and nutritional vitamin D should be interpreted with caution. These treatments are more commonly prescribed in patients with more severe disease, persistent biochemical abnormalities, or greater comorbidity burden, and thus likely reflect confounding by indication rather than direct adverse effects [20, 21]. For instance, use of non-calcium phosphate binders often indicates difficult-to-control hyperphosphatemia [18], while nutritional vitamin D may be a marker of underlying metabolic instability. Taken together, these findings suggest that PTx is associated with a consistent survival advantage in patients with severe SHPT, but that this benefit is modulated by the severity of mineral metabolism disorders and the presence of coexisting comorbidities. Optimal long-term outcomes therefore require not only appropriate selection of surgical intervention, but also comprehensive management of phosphate balance, nutritional status, and concurrent therapies.
Outcomes Related to CKD-MBD
Unlike several prior observational studies and recent meta-analyses, we did not observe a significant reduction in fracture risk after PTx, which contrasts with reports suggesting a protective skeletal effect of definitive SHPT treatment [8, 22]. The EVOLVE trial also demonstrated that cinacalcet may reduce fracture events in older dialysis patients [6]. while other studies have reported favorable changes in bone turnover markers after calcimimetic therapy [23]. The discrepancy between our findings and prior literature may reflect differences in cohort composition, dialysis-related frailty, competing mortality, follow-up duration, patient selection, residual confounding, or limitations of administrative fracture coding. Although earlier studies emphasized greater fracture reduction in women and elderly populations, our real-world ESRD cohort suggests that skeletal outcomes are influenced by multiple factors beyond PTH control alone.
Similarly, hungry bone disease, a classic complication after PTx related to rapid skeletal remineralization, was not significantly different between groups in our study [24, 25], This finding is consistent with more recent cohort data suggesting improved perioperative management and modern calcium/vitamin D supplementation may attenuate the clinical burden of postoperative hungry bone disease [26]. Our findings further suggest that with modern perioperative management and careful calcium/vitamin D supplementation, the clinical burden of hungry bone disease may be substantially reduced. For cardiovascular outcomes, we observed no significant difference in MACE between groups, consistent with prior reports that cardiovascular morbidity in ESRD is driven by multiple factors beyond PTH excess, including hypertension, diabetes, vascular calcification, and chronic inflammation. Although PTx provides clear biochemical control and may improve bone turnover, these benefits alone may be insufficient to alter the complex cardiovascular trajectory of dialysis patients. Taken together, our data indicate that PTx was associated with significant survival benefit, whereas its effects on fracture prevention and cardiovascular outcomes were less consistent in this real-world ESRD cohort than suggested by prior meta-analytic evidence.
Neurocognitive Protection
An additional finding of our study is the potential neuroprotective role of PTx. Cognitive impairment is highly prevalent in dialysis patients and is driven by multifactorial mechanisms including uremic toxin accumulation, vascular calcification, oxidative stress, and dialysis-related cerebral hypoperfusion [27-29]. Elevated PTH itself is increasingly recognized as an independent contributor to neurocognitive dysfunction, interfering with acetylcholine metabolism and synaptic transmission, and associating with structural brain changes [30, 31].
PTx was associated with a significantly lower risk of mild cognitive impairment (MCI), whereas no significant difference was observed for overall cognitive impairment or dementia. This finding contrasts with the clear survival and sepsis benefits observed with PTx, and likely reflects the multifactorial nature of neurodegeneration in end-stage renal disease (ESRD). Elevated parathyroid hormone (PTH) has been associated with cerebrovascular damage, endothelial dysfunction, and neuroinflammation, all of which contribute to white matter injury and accelerated cognitive decline in patients with advanced kidney disease [32, 33]. In this context, PTx could theoretically mitigate cognitive decline by lowering PTH levels, reducing calcium-phosphate burden, and alleviating vascular calcification and oxidative stress. Our previous result also illustrated the association between hypoalbuminemia and the cognitive impairment in dialysis patients [34]. However, the absence of a measurable effect on MCI risk in our cohort suggests that PTH reduction alone is insufficient to modify the complex interplay of uremic toxins, malnutrition, vascular injury, and amyloid dysregulation that drive neurodegeneration. A more integrated therapeutic strategy—combining PTx with optimized nutritional support, preservation of serum albumin, and interventions targeting uremic toxins—may therefore be necessary to achieve meaningful cognitive benefits in ESRD populations. Further studies should be initiated to elucidate the association of the neurodenerative disorder and secondary hyperparathyroidism.
Infection and Immunoprotection
In patients who underwent parathyroidectomy, several factors demonstrated significant associations with sepsis risk. Albumin < 4 g/dL (HR 0.49, 95% CI 0.39-0.62, P < 0.001) and hemoglobin > 9 g/dL (HR 0.48, 95% CI 0.34-0.85, P = 0.002) were associated with lower observed sepsis risk. Conversely, 25(OH)D > 30 ng/mL (HR 1.55, 95% CI 1.06-1.28, P = 0.021), ARB use (HR 2.20, 95% CI 1.49-2.20, P = 0.042), nutritional vitamin D (HR 1.96, 95% CI 1.43-1.96, P = 0.002), and non-calcium phosphate binders (HR 1.48, 95% CI 1.26-1.48, P = 0.0037) were associated with higher sepsis risk.
These findings should be interpreted with caution. Although albumin <4 g/dL was associated with a lower observed sepsis risk, this result is inconsistent with established clinical evidence showing that hypoalbuminemia is strongly associated with infection-related morbidity and mortality in hemodialysis patients [35, 36]. This discrepancy likely reflects residual confounding or selection bias rather than a true protective effect.
In contrast, the association between hemoglobin > 9 g/dL and lower sepsis risk is biologically plausible. Maintaining adequate hemoglobin levels has been associated with improved clinical outcomes [37], while lower hemoglobin levels are linked to increased hospitalization and mortality in dialysis patients [38]. This is consistent with evidence suggesting that anemia correction may improve immune function, reduce oxidative stress, and decrease adverse outcomes in ESRD populations [39, 40]. For patients undergoing PTx, adequate hemoglobin levels may therefore contribute to reduced susceptibility to infection.
In contrast, patients prescribed nutritional vitamin D or non-calcium phosphate binders showed higher sepsis risk. This likely reflects confounding by indication, as these therapies are more frequently used in patients with more severe mineral bone disorder or greater comorbidity burden. Vitamin D supplementation, although known to modulate innate immunity and induce antimicrobial peptides [41], has shown inconsistent effects on infection outcomes in CKD populations. Similarly, non-calcium phosphate binder use may identify patients with more advanced hyperphosphatemia and systemic vulnerability [42]. Taken together, these findings suggest that hemoglobin status may be associated with sepsis risk in PTx patients, whereas therapies targeting mineral metabolism may serve as markers of disease severity rather than independent risk factors.
Study Limitations
This study has several limitations. First, its retrospective design using an EMR-based database may introduce residual confounding despite rigorous propensity score matching. Certain unmeasured variables such as dialysis adequacy, nutritional status, inflammatory markers, and medication adherence were not available, which could influence outcomes. Second, diagnostic accuracy relied on ICD-10-CM coding, which may be subject to misclassification bias, particularly for cognitive impairment and sepsis. Third, laboratory data such as serum PTH trajectories, calcium-phosphate product, and vitamin D levels were incompletely available in the TriNetX dataset, limiting mechanistic insight. Finally, generalizability may be limited to healthcare systems represented in TriNetX, and unmeasured practice variation in surgical technique or CAM adherence could affect outcomes. Despite these limitations, the large sample size, robust matching, and consistent results across sensitivity and subgroup analyses strengthen the validity of our findings.
Conclusion
Parathyroidectomy is associated with improved survival compared with calcimimetics in ESRD patients with severe SHPT. Importantly, PTx also reduces the risks of cognitive impairment and sepsis, outcomes that are critical to patient quality of life yet underappreciated in prior research. While CAMs remain valuable for patients unable to undergo surgery, these findings support broader consideration of PTx as a preferred therapeutic strategy in selected populations.
Abbreviations
ESRD: End-stage renal disease
SHPT: Secondary hyperparathyroidism
PTx: Parathyroidectomy
CAMs: Calcimimetics
PTH: Parathyroid hormone
MACE: Major adverse cardiovascular events
MCI: Mild cognitive impairment
HR: Hazard ratio
CI: Confidence interval
Acknowledgements
The authors would like to thank the Core Laboratory at the Department of Research, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation and Core Facility Center, Cardinal Tien Hospital, for their technical support and for allowing the use of their facilities.
Funding
This study was supported by grants from the MOST (110-2314-B-038 -075 -MY3) and Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation (TCRD-TPE-110-02(2/3) and TCRD-TPE-111-01(3/3)) and Cardinal Tien Hospital (CTH-114-AK-NDMC-2231).
Availability of Data and Materials
The datasets analyzed during the current study were obtained from the TriNetX research network, which provides access to de-identified patient-level data from participating healthcare organizations. Due to data use agreements and privacy regulations, the raw data cannot be shared publicly. Access to TriNetX data is available upon reasonable request to TriNetX (https://trinetx.com) for researchers with an institutional license.
Author Contributions
Yi-Chou Hou: Conceptualization; Methodology; Writing - original draft; Supervision; Cai-Mei Zheng: Data curation; Formal analysis; Writing - review & editing; Ko-Lin Kuo: Resources; Investigation; Validation; Kuo-Wang Tsai: Software; Visualization; Writing - review & editing; Joshua Wang: Project administration; Data curation; Formal analysis; Cheng-Yi Wang: Resources; Investigation; Validation; Ruei-Ming Chen: Methodology; Validation; Writing - review & editing; Kuo-Cheng Lu: Supervision; Funding acquisition; Conceptualization; Writing - review; supervision.
Ethics Statement
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and was approved by the Institutional Review Board of Cardinal Tien Hospital, New Taipei City, Taiwan (approval number: CTH-114-3-5-028). The requirement for informed consent was waived owing to the retrospective nature of the study and the use of de-identified data. All procedures followed relevant guidelines and regulations to ensure patient privacy and confidentiality.
Competing Interests
The authors have declared that no competing interest exists.
References
1. Hou YC, Lu CL, Lu KC. Mineral bone disorders in chronic kidney disease. Nephrology (Carlton, Vic). 2018;23(Suppl 4):88-94
2. Wang AY, Akizawa T, Bavanandan S, Hamano T, Liew A, Lu KC. et al. 2017 kidney disease: Improving Global Outcomes (KDIGO) chronic kidney disease-Mineral and Bone Disorder (CKD-MBD) Guideline Update Implementation: Asia Summit Conference Report. Kidney Int Rep. 2019;4:1523-37
3. Yamamoto S, Jørgensen HS, Zhao J, Karaboyas A, Komaba H, Vervloet M. et al. Alkaline Phosphatase and Parathyroid Hormone Levels: International Variation and Associations with Clinical Outcomes in the DOPPS. Kidney International Reports. 2024;9:863-76
4. Hou YC, Zheng CM, Chiu HW, Liu WC, Lu KC, Lu CL. Role of Calcimimetics in Treating Bone and Mineral Disorders Related to Chronic Kidney Disease. Pharmaceuticals (Basel). 2022 15
5. Komaba H, Taniguchi M, Wada A, Iseki K, Tsubakihara Y, Fukagawa M. Parathyroidectomy and survival among Japanese hemodialysis patients with secondary hyperparathyroidism. Kidney Int. 2015;88:350-9
6. Moe SM, Abdalla S, Chertow GM, Parfrey PS, Block GA, Correa-Rotter R. et al. Effects of Cinacalcet on Fracture Events in Patients Receiving Hemodialysis: The EVOLVE Trial. J Am Soc Nephrol. 2015;26:1466-75
7. Komaba H, Hamano T, Fujii N, Moriwaki K, Wada A, Masakane I. et al. Parathyroidectomy vs Cinacalcet Among Patients Undergoing Hemodialysis. J Clin Endocrinol Metab. 2022;107:2016-25
8. Evenepoel P, Jørgensen HS. Parathyroidectomy Versus Calcimimetic: The Lower the PTH the Better? J Clin Endocrinol Metab. 2022;107:e3532-e3
9. Kurella M, Chertow GM, Luan J, Yaffe K. Cognitive impairment in chronic kidney disease. J Am Geriatr Soc. 2004;52:1863-9
10. Murray AM, Tupper DE, Knopman DS, Gilbertson DT, Pederson SL, Li S. et al. Cognitive impairment in hemodialysis patients is common. Neurology. 2006;67:216-23
11. Balkrishna A, Sinha S, Kumar A, Arya V, Gautam AK, Valis M. et al. Sepsis-mediated renal dysfunction: Pathophysiology, biomarkers and role of phytoconstituents in its management. Biomed Pharmacother. 2023;165:115183
12. Song Z, Wu C, Wang R, Gillis A, Fazendin J, Lindeman B. et al. The Effects of Parathyroidectomy vs Medical Treatments for Secondary Hyperparathyroidism in Patients Undergoing Dialysis: A Meta-Analysis. Endocr Pract. 2024;30:569-76
13. Hénaut L, Boudot C, Massy ZA, Lopez-Fernandez I, Dupont S, Mary A. et al. Calcimimetics increase CaSR expression and reduce mineralization in vascular smooth muscle cells: mechanisms of action. Cardiovasc Res. 2014;101:256-65
14. Nemeth EF. Allosteric modulators of the extracellular calcium receptor. Drug Discov Today Technol. 2013;10:e277-84
15. Itano Y, Kato S, Tsuboi M, Kasuga H, Tsuruta Y, Sato F. et al. A Prospective, Randomized Clinical Trial of Etelcalcetide in Patients Receiving Hemodialysis with Secondary Hyperparathyroidism (the DUET Trial). Kidney Int Rep. 2020;5:2168-77
16. Dörr K, Kammer M, Reindl-Schwaighofer R, Lorenz M, Prikoszovich T, Marculescu R. et al. Randomized Trial of Etelcalcetide for Cardiac Hypertrophy in Hemodialysis. Circ Res. 2021;128:1616-25
17. Shoji T, Nakatani S, Kabata D, Mori K, Shintani A, Yoshida H. et al. Comparative Effects of Etelcalcetide and Maxacalcitol on Serum Calcification Propensity in Secondary Hyperparathyroidism: A Randomized Clinical Trial. Clin J Am Soc Nephrol. 2021;16:599-612
18. Disthabanchong S, Kasempin P, Srisuwarn P, Chansomboon P, Buachum N. The impact of accessibility to non-calcium-based phosphate binders and calcimimetics on mineral outcomes in patients receiving maintenance hemodialysis: A 10-year retrospective analysis of real-world data. PLoS One. 2024;19:e0304649
19. Sánchez-González MC, López-Barea F, Bajo MA, Selgas R. Serum albumin levels, an additional factor implicated in hyperparathyroidism outcome in peritoneal dialysis: a prospective study with paired bone biopsies. Adv Perit Dial. 2006;22:198-202
20. Jamal SA, Vandermeer B, Raggi P, Mendelssohn DC, Chatterley T, Dorgan M. et al. Effect of calcium-based versus non-calcium-based phosphate binders on mortality in patients with chronic kidney disease: an updated systematic review and meta-analysis. Lancet. 2013;382:1268-77
21. Suzuki H, Kanno Y, Sugahara S, Ikeda N, Shoda J, Takenaka T. et al. Effect of Angiotensin Receptor Blockers on Cardiovascular Events in Patients Undergoing Hemodialysis: An Open-Label Randomized Controlled Trial. Am J Kidney Dis. 2008;52:501-6
22. Kongsaree N, Thanyajaroen T, Dechates B, Therawit P, Mahikul W, Ngaosuwan K. Skeletal Effect of Parathyroidectomy on Patients With Primary Hyperparathyroidism: A Systematic Review and Meta-Analysis. The Journal of Clinical Endocrinology & Metabolism. 2024;109:e1922-e35
23. Hung KC, Chang JF, Hsu YH, Hsieh CY, Wu MS, Wu MY. et al. Therapeutic Effect of Calcimimetics on Osteoclast-Osteoblast Crosslink in Chronic Kidney Disease and Mineral Bone Disease. Int J Mol Sci. 2020 21
24. Silarat P, Saeseow S, Pathumarak A, Srisuwarn P, Suvikapakornkul R, Disthabanchong S. Improved Clinical Outcomes Associated With Hungry Bone Syndrome Following Parathyroidectomy in Dialysis Patients. Endocr Pract. 2024;30:1079-88
25. Brasier AR, Nussbaum SR. Hungry bone syndrome: clinical and biochemical predictors of its occurrence after parathyroid surgery. Am J Med. 1988;84:654-60
26. Lu KC, Ma WY, Yu JC, Wu CC, Chu P. Bone turnover markers predict changes in bone mineral density after parathyroidectomy in patients with renal hyperparathyroidism. Clin Endocrinol (Oxf). 2012;76:634-42
27. Bobot M, Thomas L, Moyon A, Fernandez S, McKay N, Balasse L. et al. Uremic Toxic Blood-Brain Barrier Disruption Mediated by AhR Activation Leads to Cognitive Impairment during Experimental Renal Dysfunction. J Am Soc Nephrol. 2020;31:1509-21
28. Hsieh CC, Lu KC, Huang CL, Wang JJ, Yeh TY, Lin SM. et al. Indoxyl sulfate is associated with cognitive impairment in ESRD patients by activating the extrinsic apoptosis in the neuronal cells during differentiating process. Int J Med Sci. 2025;22:1736-49
29. Polinder-Bos HA, García DV, Kuipers J, Elting JWJ, Aries MJH, Krijnen WP. et al. Hemodialysis Induces an Acute Decline in Cerebral Blood Flow in Elderly Patients. J Am Soc Nephrol. 2018;29:1317-25
30. Hou YC, Fan YM, Huang YC, Chen RM, Wang CH, Lin YT. et al. Tc-99m TRODAT-1 SPECT is a Potential Biomarker for Restless Leg Syndrome in Patients with End-Stage. Journal of clinical medicine. 2020 9
31. Stern JE, Cardinali DP. Effect of parathyroid hormone and calcitonin on cholinergic markers in rat parathyroid gland. J Neuroendocrinol. 1995;7:689-93
32. Jorde R, Waterloo K, Saleh F, Haug E, Svartberg J. Neuropsychological function in relation to serum parathyroid hormone and serum 25-hydroxyvitamin D levels. The Tromsø study. J Neurol. 2006;253:464-70
33. Tagawa M, Hamano T, Nishi H, Tsuchida K, Hanafusa N, Fukatsu A. et al. Mineral Metabolism Markers Are Associated with Myocardial Infarction and Hemorrhagic Stroke but Not Ischemic Stroke in Hemodialysis Patients: A Longitudinal Study. PLoS One. 2014;9:e114678
34. Hou YC, Chueh TI, Lu KC, Liu YC, Chen TH, Liu SH. et al. The Ratio of Plasma Amyloid-β 1-42 over Serum Albumin Can Be a Novel Biomarker Signature for Diagnosing End-Stage Renal Disease-Associated Cognitive Impairment. J Alzheimers Dis. 2024
35. Zheng P, Jiang H, Lu H, Zhuang Y. Association of hypoalbuminemia with hospitalization and mortality in hemodialysis patients with COVID-19. Ther Apher Dial. 2025;29:250-6
36. Amaral S, Hwang W, Fivush B, Neu A, Frankenfield D, Furth S. Serum albumin level and risk for mortality and hospitalization in adolescents on hemodialysis. Clin J Am Soc Nephrol. 2008;3:759-67
37. Yang P, Yuan J, Yu L, Yu J, Zhang Y, Yuan Z. et al. Clinical significance of hemoglobin level and blood transfusion therapy in elderly sepsis patients: A retrospective analysis. The American Journal of Emergency Medicine. 2023;73:27-33
38. Kuo KL, Liu JS, Lin MH, Hsu CC, Tarng DC. Association of anemia and iron parameters with mortality among prevalent peritoneal dialysis patients in Taiwan: the AIM-PD study. Sci Rep. 2022;12:1269
39. Young EW, Wang D, Kapke A, Pearson J, Turenne M, Robinson BM. et al. Hemoglobin and Clinical Outcomes in Hemodialysis: An Analysis of US Medicare Data From 2018 to 2020. Kidney Medicine. 2023 5
40. Hung SC, Kuo KL, Tarng DC, Hsu CC, Wu MS, Huang TP. Anaemia management in patients with chronic kidney disease: Taiwan practice guidelines. Nephrology (Carlton, Vic). 2014;19:735-9
41. Liu WC, Zheng CM, Lu CL, Lin YF, Shyu JF, Wu CC. et al. Vitamin D and immune function in chronic kidney disease. Clin Chim Acta. 2015;450:135-44
42. Kidney Disease. Improving Global Outcomes CKDMBDUWG. KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney international supplements. 2017;7:1-59
Author contact
![]() Corresponding author: Kuo-Cheng Lu, MD, Professor, Division of Nephrology, Department of Medicine, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, 289 Jianguo Road, New Taipei City 23142, Taiwan, Email: kuochenglucom, Phone: +886266289779.
Corresponding author: Kuo-Cheng Lu, MD, Professor, Division of Nephrology, Department of Medicine, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, 289 Jianguo Road, New Taipei City 23142, Taiwan, Email: kuochenglucom, Phone: +886266289779.