Impact Factor ISSN: 1449-1907

 Global reach, higher impact
Global reach, higher impactInt J Med Sci 2012; 9(7):582-591. doi:10.7150/ijms.4672 This issue Cite
Research Paper
Fluoroscopic Caudal Epidural Injections in Managing Post Lumbar Surgery Syndrome: Two-Year Results of a Randomized, Double-Blind, Active-Control Trial
Laxmaiah Manchikanti1,3 ![]() , Vijay Singh2, Kimberly A. Cash3, Vidyasagar Pampati3, Sukdeb Datta4
, Vijay Singh2, Kimberly A. Cash3, Vidyasagar Pampati3, Sukdeb Datta4
1. University of Louisville, Louisville, Kentucky, USA;
2. Pain Diagnostics Associates, Niagara, WI, USA;
3. Pain Management Center of Paducah, Paducah, Kentucky, USA;
4. Laser Spine & Pain Institute, New York, NY, USA.
Received 2012-5-30; Accepted 2012-9-4; Published 2012-9-8
Abstract
Study Design: A randomized, active control, double-blind trial. Objective: To evaluate the effectiveness of fluoroscopically directed caudal epidural injections with or without steroids in managing chronic low back and lower extremity pain secondary to post lumbar surgery syndrome. Summary of Background Data: There is a paucity of evidence concerning caudal epidural injections for managing chronic persistent low back pain with or without lower extremity pain caused by post lumbar surgery syndrome.
Methods: This active control randomized study included 140 patients with 70 patients in each group. Group I received 0.5% lidocaine, 10 mL; Group II received 9 mL of 0.5% lidocaine mixed with 1 mL of 6 mg of nonparticulate betamethasone. The multiple outcome measures included the numeric rating scale, the Oswestry Disability Index 2.0, employment status, and opioid intake with assessments at 3, 6, 12, 18, and 24 months posttreatment. Primary outcome was defined as at least 50% improvement in pain and Oswestry Disability Index scores. Patients with a positive response to the first 2 procedures with at least 3 weeks of relief were considered to be successful. All others were considered as failures.
Results: Overall in Group I, 53% and 47% of the patients and in Group II, 59% and 58% of the patients, showed significant improvement with reduction in pain scores and disability index at 12 months and 24 months. In contrast, in the successful groups, significant pain relief and improvement in function were observed in 70% and 62% of Group I at one and 2 years; in 75% and 69% of Group II at one and 2 years. The results in the successful group showed that at the end of the first year patients experienced approximately 38 weeks of relief and at the end of 2 years Group I had 62 weeks and Group II had 68 weeks of relief. Overall total relief for 2 years was 48 weeks in Group I and 54 weeks in Group II. The average procedures in the successful groups were at 4 in one year and 6 at the end of 2 years.
Conclusion: Caudal epidural injections of local anesthetic with or without steroid might be effective in patients with chronic persistent low back and/or lower extremity pain in patients with post lumbar surgery syndrome.
Keywords: Chronic low back pain, post lumbar surgery syndrome, recurrent disc herniation, epidural fibrosis, spinal stenosis, caudal epidural steroid injections.
Introduction
The increasing prevalence of chronic low back pain, which is associated with exploding diagnostic and therapeutic modalities and a disproportionate increase of health care expenditures, is a major health policy issue in the United States and across the world [1-15]. Apart from multiple conservative modalities of treatments and interventional techniques, surgical interventions have been performed extensively for intervertebral disc herniation, spinal stenosis, and degenerative spondylolisthesis with stenosis [10,12,16-19].
Comparative effectiveness evidence from the Spine Patient Outcomes Research Trial (SPORT) [18] showed significant improvement in patients who had surgical interventions compared to conservative treatment modalities. The SPORT trial also showed a reoperation rate of 4% at one-year, and 10% at 4 years. Further, the literature is replete with numerous evaluations illustrating a 9.5% to 25% reoperation rate [19-28]. Martin et al [29], in a recent report, showed a mean reoperation rate of 6.1% at one-year, and 13.2% at 4 years, higher than the SPORT reoperation benchmarks. Deyo et al [30], in a report of revision surgery following operations for lumbar spinal stenosis, showed that the probability of repeat surgery at 4 years was 10.6% to 17.2%. Multiple causes shown for revision surgery in these reports were related to herniated disc, stenosis, disc degeneration, spondylolysis, spondylolisthesis, and scoliosis [29,30]. However, multiple other causes not requiring repeat surgery, or managed by interventional techniques that are responsible for continued persistent pain and disability include epidural fibrosis, sacroiliac joint pain, disc herniation, discogenic pain, spinal stenosis, and facet joint pain [11,24-28,31,32]. Even though it is widely accepted that epidural fibrosis is a major cause of complications after lumbar spine surgery, the role of peridural scarring in recurrent radicular pain has been weighed and extensively debated [32]. Ross et al [25] found that patients with extensive peridural fibrosis were 3.2 times more likely to experience recurrent radicular pain than those with less scarring. Experimental studies have provided electrophysiological evidence of neurologic disturbances caused by peridural scar formation [33]. Further, it has been shown that epidural fibrosis in the vertebral canal by invasion may cause mechanical tethering of nerve roots [34,35] and disturbances in blood flow [36] and express pro-inflammatory cytokines, which may irritate exposed dorsal root ganglion (DRG) and trigger painful responses [37]. Osteopontin also has been identified as a major player in the formation of epidural fibrosis and a mark-up DRG response to peridural scar formation [32]. Consequently, epidural fibrosis may be a causative factor in at least 20% to 36% of all cases for failed back surgery syndrome [24-26]. Further, experiments in post lumbar laminectomy syndrome in animal models have illustrated paraspinal muscle spasms, tail contractures, pain behaviors, tactile allodynia, epidural and perineural scarring, and nerve root adherence to the underlying discs and pedicle [38,39].
Epidural steroid injections and adhesiolysis are two of the most commonly utilized interventions for managing chronic, persistent low back and/or lower extremity pain in post lumbar surgery syndrome resulting from various causes, including epidural fibrosis, spinal stenosis, recurrent disc herniation, and discogenic pain without evidence of facet joint pain, radiculitis, or sacroiliac joint pain [11-15,40-44]. However, the use of epidural steroid injections has been met with not only skepticism, but also has faced significant criticism for all indications due to an alleged lack of evidence by critics, whereas supporters have described it otherwise [11-15,40-57]. There has been justification for some of the criticism, specifically in managing post lumbar surgery syndrome due to lack of quality studies with paucity of evidence. Manchikanti et al [40] published one-year results of the effectiveness of fluoroscopic caudal epidural injections for chronic low back pain with post surgery syndrome which included 140 patients, 70 patients in each group receiving local anesthetic with or without steroids. Significant improvement in pain and function was illustrated.
The current report describes a 2-year follow-up of the role of fluoroscopic caudal epidural injections in patients with chronic low back and lower extremity pain after surgical interventions with post lumbar surgery syndrome in 140 patients. The previous report of a one-year follow-up has been published [40].
Materials and Methods
The current study was conducted with the Institutional Review Board (IRB) approved protocol and registered with the U.S. Clinical Trial Registry with an assigned number of NCT00370799. The study incorporated Consolidated Standards of Reporting Trials guidelines [58] in a private interventional pain management practice and specialty referral center in the United States. This study was conducted with the internal resources of the practice without external funding from either industry or elsewhere.
Participants
One hundred and forty patients were recruited from a single pain management center and were assigned to one of 2 groups. The IRB-approved protocol and informed consent described in detail all aspects of the study and withdrawal process.
Interventions
Of the 140 patients, the 70 assigned to Group I received caudal epidural injections of local anesthetic (lidocaine 0.5%); the 70 patients assigned to Group II received caudal epidural injections of 0.5% lidocaine 9 mL mixed with 1 mL of nonparticulate betamethasone, 6 mg. A total volume of 10 mL (10 mL of lidocaine 0.5% or 9 mL of lidocaine with 1 mL of nonparticulate betamethasone), was injected, followed by an injection of 2 mL of 0.9% sodium chloride solution to flush the contents from the sacral canal.
Pre-Enrollment Evaluation
Pre-enrollment data collection included demographic data, medical, and surgical history with co-existing disease(s), radiologic investigations, physical examination, pain rating scores using the Numeric Rating Scale (NRS), functional status assessment using the Oswestry Disability Index 2.0 (ODI), work status, and opioid intake.
Inclusion and Exclusion Criteria
Criteria for inclusion in the study included only patients with a history of chronic function-limiting low back pain with or without lower extremity pain of at least 6 months duration (post surgery), with the surgery performed at least 6 months earlier; over the age of 18 years; patients who were competent to understand the study protocol and provide voluntary, written informed consent and participate in outcome measurements; evidence of a lack of diagnosed facet joint pain and failure to improve substantially with conservative management including, but not limited to, physical therapy, chiropractic manipulation, exercises, drug therapy, and bedrest.
Exclusion criteria included a positive response to controlled, comparative, local anesthetic blocks, uncontrollable or unstable opioid use, uncontrolled psychiatric disorders, uncontrolled medical illness, either acute or chronic, any conditions that could interfere with the interpretation of the outcome assessments, pregnant or lactating women, and patients with a history or potential for adverse reaction(s) to local anesthetic or steroids.
Description of Interventions
A single physician (LM) performed the caudal epidural procedures in a sterile operating room at an ambulatory surgery center. All the procedures were performed under fluoroscopy, with patients in the prone position with appropriate monitoring and intravenous sedation with midazolam and fentanyl as indicated. The epidural space was accessed and confirmed by injection of nonionic contrast medium in a sterile fashion. This was followed by injection of the appropriate mixture as assigned.
Additional Interventions
Participants received repeat caudal epidural injections if their first injection improved their physical and functional status. In addition, the repeat injections were given only when increased levels of pain were reported with deteriorating relief below 50%.
Co-Interventions
Previous drug therapy, therapeutic exercise program, and work were all continued; however, there were no specific additional interventions given to any of the patients.
Objectives
Evaluation of the effectiveness of caudal epidural injections with or without steroids in managing chronic low back and lower extremity pain secondary to post lumbar surgery syndrome.
Outcomes
The numeric rating scale (NRS) pain scale (0 - 10 scale), the Oswestry Disability Index (ODI) (0 - 50) scale, employment status, and opioid intake in terms of morphine equivalents were assessed at 3, 6, 12, 18, and 24 months posttreatment. The reliability of the NRS and ODI have been established [59,60]. A robust measure of improvement with significant pain relief and reduced disability status of 50% or more were utilized [41-44,61-69]. The opioid intake was converted into morphine equivalents [70]. Categories for employment and work status included employable, retired, over age 65, or housewife with no desire to work outside the home. Participants who, because of pain, were unemployed, on sick leave, but employed or laid off, were considered as employable. Thus, only the employable patients were considered for employment eligibility.
If a study participant received consistent relief with the first and second procedures, and at least 3 weeks with the first 2 procedures, the epidurals were considered to be successful; all others were considered failures.
Sample Size
Due to the lack of trials for estimating the sample size for post surgery syndrome, the present sample size was based on significant pain relief in lumbar disc herniation. Considering a 0.05 two-sided significance level, a power of 80%, and an allocation ratio of 1:1, 55 patients in each group were estimated [71]. Making allowances for a 20% attrition/noncompliance rate, 70 participants were determined to be required.
Randomization
Seventy patients were randomly assigned into each of the 2 groups.
Sequence Generation
Computer generated random allocations sequence by simple randomization was utilized for sequence generation.
Allocation Concealment
Participant randomization and drug preparation were performed by the operating room nurse assisting with the procedure.
Implementation
Patients willing to participate and meeting inclusion criteria were enrolled and assigned to their respective groups by one of the 3 study coordinators.
Blinding (Masking)
The physician who administered the interventions, as well as the participants, were blinded to the group assignments. Clear solution was administered in both groups. The blinding was assured by mixing the participants with patients receiving routine treatment and not informing the physician performing the procedures who was in the study.
Statistical Methods
For testing the differences in proportions, chi-squared statistic was used. Wherever the expected value was less than 5, Fisher's exact test was used; a paired t-test was used to compare the pre- and posttreatment results of average pain scores and ODI measurements at baseline versus 3, 6, 12, 18, and 24 months. T-test was performed to compare mean scores between groups. A P value of 0.05 was considered as significant. Because the outcome measures of the participants were measured at 6 points in time, repeated measures analysis of variance were performed with the post hoc analysis.
Intent-to-Treat-Analysis
An intent-to-treat-analysis was performed. Either the last follow-up data or initial data were utilized in the participants who dropped out of the study and no other data were available.
Using the last follow-up score, best case scenario, and worst case scenario, a sensitivity analysis with changes in the numeric pain scale was performed. The intent-to-treat analysis with last follow-up visit was used if there were no significant differences.
Results
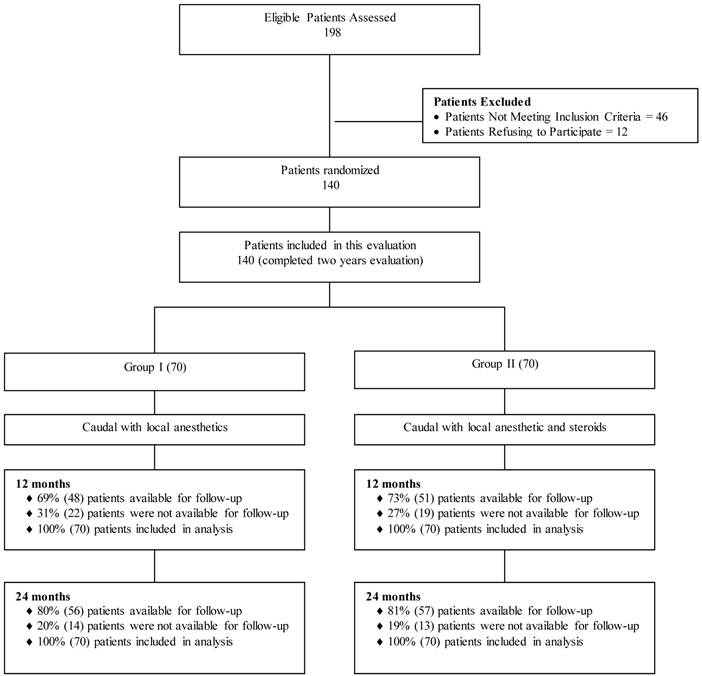
Participant Flow
The participant flow is illustrated in Figure 1.
Schematic presentation of patient flow at 2-year follow-up.
Recruitment
The recruitment period lasted from January 2007 to August 2009.
Baseline Data
Table 1 illustrates each groups' baseline demographic and clinical characteristics. Patients in Group I weighed more than Group II.
Baseline demographic and clinical data.
| Group 1 (70) | Group II (70) | P Value | ||
|---|---|---|---|---|
| Sex | Male | 39% (27) | 51% (36) | 0.126 |
| Female | 61% (43) | 49% (34) | ||
| Age | Mean ± SD | 52.4 ± 14.1 | 48.0 ± 12.3 | 0.051 |
| Weight | Mean ± SD | 200.5 ± 46.8 | 183.2 ± 41.8 | 0.023 |
| Height | Mean ± SD | 66.8 ± 3.6 | 67.1 ± 3.7 | 0.561 |
| Duration of Pain (months) | Mean ± SD | 152.1 ± 106.9 | 160.7 ± 113.3 | 0.644 |
| Onset of the Pain | Gradual | 57% (40) | 46% (32) | 0.176 |
| Injury | 43% (30) | 54% (38) | ||
| Low Back Pain Distribution | Bilateral | 69% (48) | 67% (47) | 0.176 |
| Left or Right | 31% (22) | 33% (23) | ||
| Surgical Interventions | Discectomy or Laminectomy | 48% (34) | 48% (34) | 1.000 |
| Fusion | 36% (25) | 36% (25) | ||
| Others or Combinations | 16% (11) | 16% (11) | ||
| Number of Surgeries | One | 66% (46) | 63% (44) | 0.756 |
| Two | 23% (16) | 21% (15) | ||
| > Two | 11% (8) | 16% (11) | ||
| Numeric Rating Score | Mean ± SD | 7.8 ± 1.0 | 7.8 ± 0.9 | 0.788 |
| Oswestry Disability Index | Mean ± SD | 30.3 ± 4.5 | 29.1 ± 4.5 | 0.110 |
Therapeutic Procedural Characteristics
Therapeutic procedural characteristics with average pain relief per procedure are illustrated in Table 2. The total number of procedures per 2 years was 5.7 ± 2.3 in Group I and 6.3 ± 2.2 in Group II for successful participants with relief of 62.1 ± 33.8 weeks in Group I and 67.8 ± 30.5 weeks in Group II. In contrast, in failed participants the number of injections per year was 1.3 ± 0.6 in Group I and 1.7 ± 0.8 in Group II with average relief of 2.4 ± 3.6 weeks in Group I and 2.2 ± 3.3 weeks in Group II.
Therapeutic procedural characteristics with average relief per procedure, and average total relief in weeks over a period of 2 years.
| Successful Participants | Failed Participants | All Participants | ||||
|---|---|---|---|---|---|---|
| Group I (53) | Group II (55) | Group I (17) | Group II (15) | Group I (70) | Group II (70) | |
| At One Year | ||||||
| Average number of procedures per one year | 4.0 ± 1.0 | 4.1 ± 1.0 | 1.35 ± 0.5 | 1.7 ± 0.8 | 3.4 ± 1.5 | 3.6 ± 1.4 |
| Total number of procedures in one year | 212 | 226 | 23 | 25 | 235 | 251 |
| Total relief per one year (weeks) | 38.1 ± 14.5 | 38.4 ± 13.2 | 2.4 ± 3.6 | 2.1 ± 3.3 | 29.5 ± 20.2 | 30.7 ± 19.1 |
| At Two Years | ||||||
| Average number of procedures per two years | 5.7 ± 2.3 | 6.3 ± 2.2 | 1.3 ± 0.6 | 1. 7 ± 0.8 | 4.6 ± 2.8 | 5.3 ± 2.7 |
| Total number of procedures in two years | 302 | 346 | 23 | 25 | 325 | 371 |
| Total relief per two years (weeks) | 62.1 ± 33.8 | 67.8 ± 30.5 | 2.4 ± 3.6 | 2.2 ± 3.3 | 47.6 ± 39.1 | 53.7 ± 38.3 |
| Average Relief per Procedure | ||||||
| For initial 2 procedures in weeks | 7.5 + 7.1 | 6.5 + 4.2 | 1.8 + 3.1 | 1.1 + 1.4 | 6.5 ± 7.8 | 5.5 ± 4.3 |
| After initial 2 procedures | 12.7 + 4.5 | 12.8 + 4.6 | - | 4.0 + 1.4 | 12.7 + 4.5 | 12.7 + 4.7 |
| All procedures | 10.9 + 6.5 | 10.8 + 5.3 | 1.8 + 3.1 | 1.3 + 1.6 | 10.3 + 6.8 | 10.1 + 5.7 |
Successful participant - At least ≥ 3 weeks relief with first 2 procedures.
To be considered successful, the first 2 procedures had to provide at least 3 weeks of relief.
Outcomes
Pain Relief and Functional Assessment
Table 3 presents the results of repeated measures analysis. Regarding pain scores, there were significant differences within groups by time (P = 0.0000). In the Oswestry Disability Index for functional status, there were significant differences in summary scores within group by time (P = 0.000).
Comparison of Numeric Rating Scale for pain and Oswestry Disability Index score summaries at four time points.
| Time Points | Numeric Pain Rating Score (Mean ± SD) | Oswestry Disability Index (Mean ± SD) | ||
|---|---|---|---|---|
| Group I (70) | Group II (70) | Group I (70) | Group II (70) | |
| Baseline | 7.8 ± 1.0 | 7.8 ± 0.9 | 30.3 ± 4.5 | 29.1 ± 4.5 |
| 3 months | 4.2* ± 1.8 (66%) | 4.1* ± 1.7 (69%) | 17.6* ± 6.3 (56%) | 16.8* ± 6.8 (57%) |
| 6 months | 4.3* ± 1.9 (60%) | 4.1* ± 1.7 (66%) | 17.6* ± 6.9 (56%) | 16.3* ± 7.0 (63%) |
| 12 months | 4.5* ± 1.9 (56%) | 4.2* ± 1.7 (61%) | 17.7* ± 6.9 (54%) | 16.5* ± 7.0 (61%) |
| 18 months | 4.6* ± 1.9 (50%) | 4.1* ± 1.8 (61%) | 17.9* ± 7.0 (50%) | 16.6* ± 6.9 (57%) |
| 24 months | 4.4* ± 1.9 (49%) | 4.2* ± 1.8 (56%) | 17.8* ± 7.2 (49%) | 16.6* ± 7.0 (56%) |
| Group Difference | 0.376 | 0.180 | ||
| Baseline vs follow-up points | 0.000 | 0.000 | ||
| Group by Time Interaction* | 0.310 | 0.896 | ||
Percentages in parenthesis illustrates proportion with significant pain relief (≥ 50%) from baseline
* indicates significant difference with baseline values (P < 0.05)
* Group by Time Interaction - There were no significant difference between groups at 3 months, 6 months, 12 months, 18 months and 24 months.
A post-hoc analysis indicates that all the mean differences between baseline and with other time point's scores were significant at the 0.05 level.
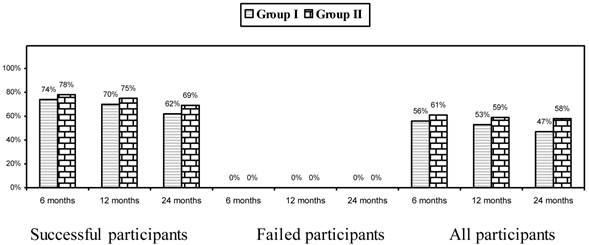
Combined Pain Relief and Functional Status
Figure 2 illustrates proportion of patients with significant reduction (≥ 50%) in NRS scores and ODI.
Proportion of patients with significant reduction in Numeric Rating Score and Oswestry Disability Index (≥ 50% reduction from baseline).
Employment Characteristics
Employment characteristics are illustrated 12 patients in Group I and 17 patients in Group II eligible for employment with 9 patients in Group I and 13 patients in Group II employed at baseline. At the end of 1 and 2 years, 13 patients were employed in Group I, whereas in Group II, 15 patients at the end of 1 year and 14 patients at the end of 2 years were employed, with employment available for all those who were eligible.
Opioid Intake
Opioid intake (characteristics with increases and decreases illustrated decrease in intake from baseline in both groups, without changes among the groups.
Changes in Weight
Changes in body weight are illustrated in Table 4.
Characteristics weight monitoring.
| Weight (lbs) | Group I (70) | Group II (70) | P value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Weight at Beginning | 200.5 ± 46.8 | 183.2 ± 41.8 | 0.023 |
| At One Year | |||
| Weight at One Year | 197.0 ± 47.7 | 180.2 ± 42.1 | 0.028 |
| Change | -3.5 ± 12.6 | -3.0 ± 9.3 | 0.808 |
| Lost Weight | 43% (30) | 56% (39) | 0.102 |
| No Change | 34% (24) | 18% (13) | |
| Gained Weight | 23% (16) | 26% (18) | |
| At Two Years | |||
| Weight at Two Years | 196.0 ± 49.9 | 181.6 ± 42.2 | 0.067 |
| Change | -3.2 ± 16.2 | -1.6 ± 15.8 | 0.562 |
| Lost Weight | 44% (31) | 49% (34) | 0.463 |
| No Change | 26% (18) | 17% (12) | |
| Gained Weight | 30% (21) | 34% (24) |
Adverse Events
No major adverse events were reported over the 2-year study period in any of the 696 procedures performed in the140 participants.
Discussion
This relatively large, randomized, double-blind, active control trial of fluoroscopic caudal epidural injections with or without steroids in 140 patients with chronic, persistent low back and lower extremity pain secondary to post lumbar surgery syndrome showed clinically meaningful and significant improvement with pain and functional status at the end of one and 2 years. The results of this practical evaluation performed in a nonacademic private practice setting simulating practice patterns illustrates that in carefully selected patients, who do not have facet joint pain, those judged as successful participants (i.e., who responded to the first 2 procedures with at least 3 weeks of relief), combined pain relief and improvement in functional status was observed in 62% in Group I and 69% in Group II at the 2-year follow-up. Further, the overall improvement was also significant when all participants were included with 47% of the patients showing improvement in Group I and 58% of the patients showing improvement in Group II at the end of 2 years. Thus, this study confirms that caudal epidural injections in appropriately selected patients with post lumbar surgery syndrome are a successful modality for managing this chronic, recalcitrant condition. Further, the response was similar in patients receiving local anesthetic only or local anesthetic and steroid combination with nonparticulate betamethasone. There was no significant difference in the total relief over a period of 2 years with 62.1 ± 33.8 weeks in Group I and 67.8 ± 30.5 weeks in Group II in the successful groups. Further, the average relief per procedure for the initial 2 procedures, as well as subsequent procedures and overall procedures over the period of 2 years was similar in both groups of patients with respect to overall results.
The average number of procedures at the end of one year was approximately 3.5 and after 2 years, the average number was 5 in both groups. However, in the successful groups, the number of treatments were approximately 4 and 6 at the end of one and 2 years.
The literature is replete with multiple studies and systematic reviews in favor and against epidural injections [11-13,46-64,71]. Particularly, there are no studies evaluating the effectiveness of fluoroscopically directed caudal epidural injections under optimal conditions of contemporary interventional pain management practice in a large number of patients. Multiple studies have been criticized, most importantly for their design and their inability to confirm the location of the injectate by not using fluoroscopy [11,58,60,62,63,72-74]. Multiple systematic reviews have been criticized for their methodology by evaluating studies inappropriately, thus, reaching inaccurate conclusions based on inappropriate evidence synthesis [11-13,44-64,71,75].
In a systematic review by Conn et al [73] of randomized and nonrandomized studies of caudal epidural injections for managing chronic low back pain of post-surgery syndrome along with other conditions, only one trial's preliminary data met inclusion criteria of long-term follow-up of at least 6 months along with the use of fluoroscopic visualization [74]. They concluded that due to the paucity of literature, the evidence was Level II-2. However, other systematic reviews have combined multiple approaches into one category, with the majority of them performed blindly without fluoroscopy [11-13].
This study may be criticized for its lack of a placebo group. However, there are numerous difficulties related to having a placebo group in interventional techniques studies. Further, placebo experimentation has yielded highly variable results. This is because the injection of an inactive compound into an active structure was performed by those who lack an understanding of placebo and nocebo in clinical trials [75-83]. Properly designed placebo control illustrated appropriate results [83]. In addition, arguments may be made with regards to local anesthetic being placebo [78]; however, local anesthetic and steroids both have been shown to exert similar effects in experimental and clinical studies [45-52,68-71,83-88]. The mechanisms of action of epidural steroids and local anesthetics have been discussed in multiple manuscripts [11,40,42-44].
In summary, the evidence shown in this 2-year evaluation of a randomized, active control, double-blind trial demonstrates that caudal epidural injections in patients with post lumbar surgery syndrome with chronic, persistent, low back and/or lower extremity pain provides significant relief. Consequently, selected patients may be offered caudal epidural injections with or without steroids on a long-term basis.
Conclusion
The two-year results of this randomized, double-blind, active controlled trial of epidural effectiveness for post lumbar surgery syndrome illustrates 47% of patients receiving local anesthetic and 58% of patients receiving local anesthetic and steroids showed significant improvement in both pain relief and functional status. There was no statistically significant difference in outcome between the 2 groups. However, the data from the successful groups showed improvement in 62% of patients in Group I and 69% of patients in Group II.
Acknowledgements
The authors wish to thank Sekar Edem for assistance in the search of the literature, Tom Prigge, MA for manuscript review, and Tonie M. Hatton and Diane E. Neihoff, transcriptionists, for their assistance in preparation of this manuscript.
Competing Interests
The authors have declared that no competing interest exists.
References
1. Hoy D, Brooks P, Blyth F. et al. The epidemiology of low back pain. Best Pract Res Clin Rheumatol. 2010;24:769-81
2. Martin BI, Turner JA, Mirza SK. et al. Trends in health care expenditures, utilization, and health status among US adults with spine problems, 1997-2006. Spine (Phila Pa 1976). 2009;24:2077-84
3. Freburger JK, Holmes GM, Agans RP. et al. The rising prevalence of chronic low back pain. Arch Intern Med. 2009;169:251-8
4. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research, June 29, 2011. Institute of Medicine (IOM) Consensus Report. http://www.iom.edu/~/media/Files/Report%20Files/2011/Relieving-Pain-in-America-A-Blueprint-for-Transforming-Prevention-Care-Education-Research/Pain%20Research%202011%20Report%20Brief.pdf
5. Manchikanti L, Fellows B, Ailinani H. et al. Therapeutic use, abuse, and nonmedical use of opioids: a ten-year perspective. Pain Physician. 2010;13:401-35
6. Ivanova JI, Birnbaum HG, Schiller M. et al. Real-world practice patterns, health-care utilization, and costs in patients with low back pain: the long road to guideline-concordant care. Spine J. 2011;11:622-32
7. Luo X, Pietrobon R, Sun SX. et al. Estimates and patterns of direct health care expenditures among individuals with back pain in the United States. Spine (Phila Pa 1976). 2004;29:79-86
8. Rubinstein SM, van Middelkoop M, Assendelft WJ. et al. Spinal manipulative therapy for chronic low-back pain: an update of a Cochrane review. Spine (Phila Pa 1976). 2011;36:E825-46
9. van Middelkoop M, Rubinstein SM, Kuijpers T. et al. A systematic review on the effectiveness of physical and rehabilitation interventions for chronic non-specific low back pain. Eur Spine J. 2011;20:19-39
10. Deyo RA, Mirza SK, Turner JA. et al. Overtreating chronic back pain: time to back off? J Am Board Fam Med. 2009;22:62-8
11. Manchikanti L, Boswell MV, Singh V. et al. Comprehensive evidence-based guidelines for interventional techniques in the management of chronic spinal pain. Pain Physician. 2009;12:699-802
12. Chou R, Huffman L. Guideline for the Evaluation and Management of Low Back Pain: Evidence Review. Glenview, IL: American Pain Society. 2009
13. Staal JB, de Bie RA, de Vet HC. et al. Injection therapy for subacute and chronic low back pain: an updated Cochrane review. Spine (Phila Pa 1976). 2009;34:49-59
14. Abbott Zi, Nai KV, Allen RR. et al. Utilization characteristics of spinal interventions. Spine J. 2012;1:35-43
15. Manchikanti L, Pampati V, Boswell MV. et al. Analysis of the growth of epidural injections and costs in the Medicare population: a comparative evaluation of 1997, 2002, and 2006 data. Pain Physician. 2010;13:199-212
16. Jacobs WC, van Tulder M, Arts M. et al. Surgery versus conservative management of sciatica due to a lumbar herniated disc: a systematic review. Eur Spine J. 2011;20:513-22
17. Rajaee SS, Bae HW, Kanim LE. et al. Spinal fusion in the United States: analysis of trends from 1998 to 2008. Spine (Phila Pa 1976). 2012;37:67-76
18. Tosteson AN, Tosteson TD, Lurie JD. et al. Comparative effectiveness evidence from the spine patient outcomes research trial: Surgical versus nonoperative care for spinal stenosis, degenerative spondylolisthesis, and intervertebral disc herniation. Spine (Phila Pa 1976). 2011;36:2061-8
19. Deyo RA, Mirza SK, Martin BI. et al. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA. 2010;303:1259-65
20. Davis H. Increasing rates of cervical and lumbar spine surgery in the United States, 1979-1990. Spine (Phila Pa 1976). 1994;19:1117-23
21. Hu RW, Jaglal S, Axcell T. et al. A population-based study of reoperations after back surgery. Spine (Phila Pa 1976). 1997;22:2265-70
22. Malter AD, McNeney B, Loeser JD. et al. 5-year reoperation rates after different types of lumbar spine surgery. Spine (Phila Pa 1976). 1998;23:814-20
23. Keskimäki I, Seitsalo S, Osterman H. et al. Reoperations after lumbar disc surgery: a population-based study of regional and interspecialty variations. Spine (Phila Pa 1976). 2000;25:1500-8
24. Waddell G, Kummel EG, Lotto WN. et al. Failed lumbar disc surgery and repeat surgery following industrial injury. J Bone Joint Surg Am. 1979;61:201-7
25. Ross JS, Robertson JT, Frederickson RC. et al. Association between peridural scar and recurrent radicular pain after lumbar discectomy: magnetic resonance evaluation. Neurosurgery. 1996;38:855-63
26. Fritsch EW, Heisel J, Rupp S. The failed back surgery syndrome. Reasons, intraoperative findings, and long-term results: a report of 182 operative treatments. Spine (Phila Pa 1976). 1996;21:626-33
27. Osterman H, Sund R, Seitsalo S. et al. Risk of multiple reoperations after lumbar discectomy: a population-based study. Spine (Phila Pa 1976). 2003;28:621-7
28. Law JD, Lehman RAW, Kirsch WM. Reoperation after lumbar intervertebral disc surgery. J Neurosurg. 1978;48:259-63
29. Martin BI, Mirza SK, Flum DR. et al. Repeat surgery after lumbar decompression for herniated disc: the quality implications of hospital and surgeon variation. Spine J. 2011 [Epub ahead of print]
30. Deyo RA, Martin BI, Kreuter W. et al. Revision surgery following operations for lumbar stenosis. J Bone Joint Surg Am. 2011;93:1979-86
31. Manchikanti L, Manchukonda R, Pampati V. et al. Prevalence of facet joint pain in chronic low back pain in postsurgical patients by controlled comparative local anesthetic blocks. Arch Phys Med Rehabil. 2007;88:449-55
32. Brzezicki G, Jankowski R, Blok T, Klimczak A. et al. Postlaminectomy osteopontin expression and associated neurophysiological findings in rat peridural scar model. Spine (Phila Pa 1976). 2011;36:378-85
33. Jou IM, Tai TW, Tsai CL. et al. Spinal somatosensory evoked potential to evaluate neurophysiologic changes associated with postlaminotomy fibrosis: an experimental study. Spine (Phila Pa 1976). 2007;32:2111-8
34. Alkalay RN, Kim DH, Urry DW. et al. Prevention of postlaminectomy epidural fibrosis using bioelastic materials. Spine (Phila Pa 1976). 2003;28:1659-65
35. Ozer AF, Oktenoglu T, Sasani M. et al. Preserving the ligamentum flavum in lumbar discectomy: a new technique that prevents scar tissue formation in the first 6 months post surgery. Neurosurgery. 2006;59:ONS126-33
36. Cooper RG, Freemont AJ, Hoyland JA. et al. Herniated intervertebral disc-associated periradicular fibrosis and vascular abnormalities occur without inflammatory cell infiltration. Spine (Phila Pa 1976). 1995;20:591-8
37. Schimizzi AL, Massie JB, Murphy M. et al. High-molecular-weight hyaluronan inhibits macrophage proliferation and cytokine release in the early wound of a preclinical postlaminectomy rat model. Spine J. 2006;6:550-6
38. Massie JB, Huang B, Malkmus S. et al. A preclinical post laminectomy rat model mimics the human post laminectomy syndrome. J Neurosci Methods. 2004;137:283-9
39. Haq I, Cruz-Almeida Y, Siqueira EB. et al. Postoperative fibrosis after surgical treatment of the porcine spinal cord: a comparison of dural substitutes. Invited submission from the Joint Section Meeting on Disorders of the Spine and Peripheral Nerves, March 2004. J Neurosurg Spine. 2005;2:50-4
40. Manchikanti L, Singh V, Cash KA, et al Management of pain of post lumbar surgery syndrome. one-year results of a randomized, double-blind, active controlled trial of fluoroscopic caudal epidural injections. Pain Physician. 2010;13:509-21
41. Manchikanti L, Pampati V, Cash KA. Protocol for evaluation of the comparative effectiveness of percutaneous adhesiolysis and caudal epidural steroid injections in low back and/or lower extremity pain without post surgery syndrome or spinal stenosis. Pain Physician. 2010;13:E91-110
42. Manchikanti L, Singh V, Cash KA. et al. A randomized, controlled, double-blind trial of fluoroscopic caudal epidural injections in the treatment of lumbar disc herniation and radiculitis. Spine (Phila Pa 1976). 2011;36:1897-1905
43. Manchikanti L, Cash RA, McManus CD. et al. Fluoroscopic caudal epidural injections with or without steroids in managing pain of lumbar spinal stenosis: one year results of randomized, double-blind, active-controlled trial. J Spinal Disord. 2011 [Epub ahead of print]
44. Manchikanti L, Cash KA, McManus CD. et al. One year results of a randomized, double-blind, active controlled trial of fluoroscopic caudal epidural injections with or without steroids in managing chronic discogenic low back pain without disc herniation or radiculitis. Pain Physician. 2011;14:25-36
45. Manchikanti L, Falco FJE, Boswell MV. et al. Facts, fallacies, and politics of comparative effectiveness research: part 1. Basic considerations. Pain Physician. 2010;13:E23-54
46. Manchikanti L, Falco FJE, Boswell MV. et al. Facts, fallacies, and politics of comparative effectiveness research: part 2. Implications for interventional pain management. Pain Physician. 2010;13:E55-79
47. Manchikanti L, Falco FJ, Benyamin RM. et al. The impact of comparative effectiveness research on interventional pain management: evolution from Medicare Modernization Act to Patient Protection and Affordable Care Act and the Patient-Centered Outcomes Research Institute. Pain Physician. 2011;14:E249-82
48. Ackerman WE 3rd, Ahmad M. The efficacy of lumbar epidural steroid injections in patients with lumbar disc herniations. Anesth Analg. 2007;104:1217-22
49. Manchikanti L, Datta S, Derby R. et al. A critical review of the American Pain Society clinical practice guidelines for interventional techniques: part 1. Diagnostic interventions. Pain Physician. 2010;13:E141-74
50. Manchikanti L, Datta S, Gupta S. et al. A critical review of the American Pain Society clinical practice guidelines for interventional techniques: part 2. Therapeutic interventions. Pain Physician. 2010;13:E215-64
51. Manchikanti L, Singh V, Boswell MV. Interventional pain management at crossroads: the perfect storm brewing for a new decade of challenges. Pain Physician. 2010;13:E111-40
52. Benyamin RM, Datta S, Falco FJE. A perfect storm in interventional pain management: regulated, but unbalanced. Pain Physician. 2010;13:109-16
53. Sayegh FE, Kenanidis EI, Papavasiliou KA. et al. Efficacy of steroid and nonsteroid caudal epidural injections for low back pain and sciatica: a prospective, randomized, double-blind clinical trial. Spine (Phila Pa 1976). 2009;34:1441-7
54. Iversen T, Solberg TK, Romner B. et al. Effect of caudal epidural steroid or saline injection in chronic lumbar radiculopathy: multicentre, blinded, randomised controlled trial. BMJ. 2011;343:d5278
55. Manchikanti L, Falco FJE, Boswell MV. et al. Facts, fallacies, and politics of comparative effectiveness research: part 1. Basic considerations. Pain Physician. 2010;13:E23-54
56. Chou R, Atlas SJ, Loeser JD, Rosenquist RW, Stanos SP. Guideline warfare over interventional therapies for low back pain: can we raise the level of discourse? J Pain. 2011;12:833-9
57. Manchikanti L, Benyamin RM, Falco FJE, Caraway DL, Datta S, Hirsch JA. Guidelines warfare over interventional techniques: is there a lack of discourse or straw man? Pain Physician. 2012;15:E1-E26
58. Altman DG, Schulz KF, Moher D, et al; CONSORT GROUP (Consolidated Standards of Reporting Trials). The revised CONSORT statement for reporting randomized trials: Explanation and elaboration. Ann Intern Med. 2001;134:663-94
59. Manchikanti L, Benyamin RM, Helm S. et al. Evidence-based medicine, systematic reviews, and guidelines in interventional pain management: part 3: Systematic reviews and meta-analyses of randomized trials. Pain Physician. 2009;12:35-72
60. Fairbank JC, Pynsent PB. The Oswestry Disability Index. Spine (Phila Pa 1976). 2000;25:2940-52
61. Manchikanti L, Singh V, Falco FJ. et al. Comparative outcomes of a 2-year follow-up of cervical medial branch blocks in management of chronic neck pain: a randomized, double-blind controlled trial. Pain Physician. 2010;13:437-50
62. Manchikanti L, Singh V, Falco FJ. et al. Evaluation of lumbar facet joint nerve blocks in managing chronic low back pain: a randomized, double-blind, controlled trial with a 2-year follow-up. Int J Med Sci. 2010;7:124-35
63. Manchikanti L, Singh V, Falco FJ. et al. Comparative effectiveness of a one-year follow-up of thoracic medial branch blocks in management of chronic thoracic pain: a randomized, double-blind active controlled trial. Pain Physician. 2010;13:535-48
64. Manchikanti L, Cash KA, Pampati V. et al. Cervical epidural injections in chronic discogenic neck pain without disc herniation or radiculitis: preliminary results of a randomized, double-blind, controlled trial. Pain Physician. 2010;13:E265-78
65. Manchikanti L, Cash KA, Pampati V. et al. The effectiveness of fluoroscopic cervical interlaminar epidural injections in managing chronic cervical disc herniation and radiculitis: preliminary results of a randomized, double-blind, controlled trial. Pain Physician. 2010;13:223-36
66. Manchikanti L, Cash KA, McManus CD. et al. A preliminary report of a randomized double-blind, active controlled trial of fluoroscopic thoracic interlaminar epidural injections in managing chronic thoracic pain. Pain Physician. 2010;13:E357-69
67. Manchikanti L, Singh V, Falco FJE. et al. Evaluation of the effectiveness of lumbar interlaminar epidural injections in managing chronic pain of lumbar disc herniation or radiculitis: a randomized, double-blind, controlled trial. Pain Physician. 2010;13:343-55
68. Manchikanti L, Cash KA, McManus CD. et al. Preliminary results of a randomized, double-blind, controlled trial of fluoroscopic lumbar interlaminar epidural injections in managing chronic lumbar discogenic pain without disc herniation or radiculitis. Pain Physician. 2010;13:E279-92
69. Manchikanti L, Cash KA, McManus CD. et al. Lumbar interlaminar epidural injections in central spinal stenosis: preliminary results of a randomized, double-blind, active control trial. Pain Physician. 2012;15:51-63
70. Pereira J, Lawlor P, Vigano A. et al. Equianalgesic does ratios for opioids. a critical review and proposals for long-term dosing. J Pain Symptom Manage. 2001;22:672-87
71. Browner WS, Newman TB, Cummings SR. et al. Estimating sample size and power. In: (ed.) Hulley Sb, Cummings SR, Browner WS. et al. Designing Clinical Research: An Epidemiologic Approach, 2nd ed. Philadelphia, PA: Lippincott, Williams & Wilkins. 2001:65-84
72. Gupta S, Ward S, Munglani R. et al. Letter to the Editor re: Iversen T, Solberg TK, Romner B, et al. Effect of caudal epidural steroid or saline injection in chronic lumbar radiculopathy: multicentre, blinded, randomised controlled trial. BMJ. 2011;343:d5278
73. Conn A, Buenaventura RM, Datta S. et al. Systematic review of caudal epidural injections in the management of chronic low back pain. Pain Physician. 2009;12:109-35
74. Manchikanti L, Singh V, Cash KA. et al. Preliminary results of a randomized, equivalence trial of fluoroscopic caudal epidural injections in managing chronic low back pain: part 3--Post surgery syndrome. Pain Physician. 2008;11:817-31
75. Carette S, Leclaire R, Marcoux S. et al. Epidural corticosteroid injections for sciatica due to herniated nucleus pulposus. N Engl J Med. 1997;336:1634-40
76. Karppinen J, Malmivaara A, Kurunlahti M. et al. Periradicular infiltration for sciatica: a randomized controlled trial. Spine (Phila Pa 1976). 2001;26:1059-67
77. Manchikanti L, Giordano J, Fellows B. et al. Placebo and nocebo in interventional pain management: a friend or a foe--or simply foes? Pain Physician. 2011;14:E157-75
78. Smuck M, Levin JH. Re: Manchikanti L, Singh V, Falco FJ, et al. Cervical medial branch blocks for chronic cervical facet joint pain: a randomized, double-blind, controlled trial with one-year follow-up. Spine (Phila Pa 1976). 2008;33:1813-20
79. Indahl A, Kaigle AM, Reikeräs O. et al. Interaction between the porcine lumbar intervertebral disc, zygapophysial joints, and paraspinal muscles. Spine (Phila Pa 1976). 1997;22:2834-40
80. Indahl A, Kaigle A, Reikerås O. et al. Electromyographic response of the porcine multifidus musculature after nerve stimulation. Spine (Phila Pa 1976). 1995;20:2652-8
81. Pham Dang C, Lelong A, Guilley J. et al. Effect on neurostimulation of injectates used for perineural space expansion before placement of a stimulating catheter: normal saline versus dextrose 5% in water. Reg Anesth Pain Med. 2009;34:398-403
82. Tsui BC, Kropelin B, Ganapathy S. et al. Dextrose 5% in water: Fluid medium for maintaining electrical stimulation of peripheral nerves during stimulating catheter placement. Acta Anaesthesiol Scand. 2005;49:1562-5
83. Ghahreman A, Ferch R, Bogduk N. The efficacy of transforaminal injection of steroids for the treatment of lumbar radicular pain. Pain Med. 2010;11:1149-68
84. Pasqualucci A, Varrassi G, Braschi A. et al. Epidural local anesthetic plus corticosteroid for the treatment of cervical brachial radicular pain: single injection versus continuous infusion. Clin J Pain. 2007;23:551-7
85. Tachihara H, Sekiguchi M, Kikuchi S. et al. Do corticosteroids produce additional benefit in nerve root infiltration for lumbar disc herniation? Spine (Phila Pa 1976). 2008;33:743-7
86. Sato C, Sakai A, Ikeda Y. et al. The prolonged analgesic effect of epidural ropivacaine in a rat model of neuropathic pain. Anesth Analg. 2008;106:313-20
87. Hayashi N, Weinstein JN, Meller ST. et al. The effect of epidural injection of betamethasone or bupivacaine in a rat model of lumbar radiculopathy. Spine (Phila Pa 1976). 1998;23:877-85
88. Lee HM, Weinstein JN, Meller ST. et al. The role of steroids and their effects on phospholipase A2. an animal model of radiculopathy. Spine (Phila Pa 1976). 1998;23:1191-6
Author contact
![]() Corresponding author: Laxmaiah Manchikanti, M.D. 2831 Lone Oak Road, Paducah, Kentucky 42003, Phone: 270-554-8373 Fax: 270-554-8987 E-mail: drlmcom.
Corresponding author: Laxmaiah Manchikanti, M.D. 2831 Lone Oak Road, Paducah, Kentucky 42003, Phone: 270-554-8373 Fax: 270-554-8987 E-mail: drlmcom.