Impact Factor ISSN: 1449-1907

 Global reach, higher impact
Global reach, higher impactInt J Med Sci 2012; 9(6):472-479. doi:10.7150/ijms.4637 This issue Cite
Research Paper
Clinical Application of Pharmacogenetic-Based Warfarin-Dosing Algorithm in Patients of Han Nationality after Rheumatic Valve Replacement: A Randomized and Controlled Trial
MingSong Wang1#, XiLong Lang2#, ShiTao Cui3 ![]() , Ke Fei4
, Ke Fei4 ![]() , LiangJian Zou2, Jia Cao5, LiangXu Wang5, ShengHui Zhang5, XinTian Wu5, YiLing Wang5, Qiang Ji6
, LiangJian Zou2, Jia Cao5, LiangXu Wang5, ShengHui Zhang5, XinTian Wu5, YiLing Wang5, Qiang Ji6 ![]()
1. Department of Thoracic Cardiovascular Surgery, Xinhua Hospital of Shanghai Jiaotong University School of Medicine, Shanghai 200092, P.R. China.
2. Department of Cardiothoracic Surgery, Changhai Hospital, Second Military Medical University, Shanghai 200433, P.R. China.
3. Department of Emergency Surgery, Ninth People's Hospital of Shanghai Jiaotong University School of Medicine, Shanghai 200072, P.R. China.
4. Department of Thoracic Surgery, Pulmonary Hospital of Tongji University, Shanghai 200433, P.R. China.
5. Department of Thoracic Cardiovascular Surgery, Tenth People's Hospital of Tongji University, Shanghai 200072, P.R. China.
6. Department of Thoracic Cardiovascular Surgery, Tongji Hospital of Tongji University, Shanghai 200065, P.R. China.
# Contributed equally as the co-first author.
Received 2012-5-23; Accepted 2012-7-24; Published 2012-8-10
Abstract
Background The polymorphisms of VKORC1 and CYP2C9 play increasingly important roles in the inter-individual variability in warfarin dose. This study aimed to evaluate the feasibility of clinical application of pharmacogenetic-based warfarin-dosing algorithm in patients of Han nationality with rheumatic heart disease after valve replacement in a randomized and controlled trial. Methods One hundred and one consecutive patients of Han nationality with rheumatic heart disease undergoing valve surgery were enrolled and randomly assigned to an experimental group (n=50, based on CYP2C9 and VKORC1 genotypes, pharmacogenetic-based “predicted warfarin dose” for 3 days and then was adjusted to INR until stable warfarin maintenance dose) or a control group (n=51, 2.5mg/d for 3 days and then was adjusted to INR until stable warfarin maintenance dose). All included patients were followed for 50 days after initiation of warfarin therapy. The primary end-point was the time to reach a stable warfarin maintenance dose. Results During the follow-up, 84.0% patients in the experimental group and 58.8% patients in the control group received warfarin maintenance dose. Compared with control group, patients in the experimental group had shorter mean time elapse from initiation of warfarin therapy until warfarin maintenance dose (27.5±1.8 d versus 34.7±1.8 d, p<0.001). Cox regression revealed that group (HR for experimental versus control group: 1.568, 95%CI 1.103-3.284) and age were two significant variables related to the time elapse from initiation of warfarin therapy until warfarin maintenance dose. The predicted warfarin maintenance dose was prominently correlated with the actual warfarin maintenance dose (r=0.684, p<0.001). Conclusion: Based on CYP2C9 and VKORC1 genotypes, the pharmacogenetic-based warfarin-dosing algorithm may shorten the time elapse from initiation of warfarin therapy until warfarin maintenance dose. It is feasible for the clinical application of the pharmacogenetic-based warfarin-dosing algorithm in patients of Han nationality with rheumatic heart disease after valve replacement.
Keywords: Pharmacogenetics, Individualized warfarin therapy, Rheumatic valve surgery, Trial.
Introduction
With the development of the pharmacogenomics and the elucidation of pharmacological molecular mechanism of warfarin, the polymorphisms of VKORC1 and CYP2C9 play increasingly important roles in the inter-individual variability in warfarin dose [1-3]. The polymorphism of VKORC1 contributed 6-37% towards individual variability in warfarin dose, and CYP2C9 5-22% [3, 4]. Previous studies [1-4] reported that patients with VKORC1 6484TT genotype required a lower warfarin maintenance dose compared to VKORC1 6484TC genotype or VKORC1 6484CC genotype, and patients with CYP2C9*1/*1 genotype required a higher warfarin maintenance dose compared to CYP2C9*1/*3 genotype or CYP2C9*3/*3 genotype. So, researchers suggested that a warfarin-dosing algorithm to predict warfarin maintenance dose should be established to improve the efficacy and safety of warfarin therapy, on the basis of not only non-genetic factors but also genetic factors. Previous studies [1-4] concentrated mainly on establishing genetic-based warfarin-dosing algorithm, with few studies focusing on verifying these algorithms and evaluating its clinical value. In addition, due to ethnic differences, we should consider whether established non-Han-population-based warfarin-dosing algorithms were applied to Han population. Therefore, it is necessary to evaluate the clinical application of the pharmacogenetic-based warfarin-dosing algorithm in patients of Han nationality undergoing rheumatic valve replacement.
In this study, we evaluated the feasibility of the clinical application of the pharmacogenetic-based (based on CYP2C9 and VKORC1 genotypes) warfarin-dosing algorithm to predict warfarin maintenance dose in patients of Han nationality with rheumatic heart disease undergoing mechanical valve replacement in a randomized and controlled trial.
Materials and methods
General data
The study was approved by the hospital's ethics review committee and registered on Chinese Clinical Trial Registry (ChiCTR) site (http://www.chictr.org, number ChiCTR-TRC-11001852). This study protocol was consistent with the spirit of the Declaration of Helsinki. Informed consent was obtained from all participants.
Subjects
Han patients with rheumatic heart disease were referred to our unit at least 2 days before surgery. All patients received preoperative electrocardiogram, chest X-ray film and echocardiography with patients over 45 years old receiving preoperative coronary artery angiography.
Eligible patients were at least 18 years old, scheduled for single or double mechanical prosthetic valve replacement, had not used any other drugs known to be related to CYP2C9 and VKORC1, and had been given dietary advice to avoid foods that may interfere with warfarin metabolism. In addition, inclusive patients did not use warfarin in the past three months and the baseline international normalized ratio (INR) values were within the normal range from 0.8 to 1.2.
Women who were pregnant, lactating, or of child-bearing potential; pathological obesity; concomitant any malignancy, chronic hepatic or kidney disease, any thyroid disease, any hematological disease or history of bleeding, and infective endocarditis; any contraindication of warfarin; those participating in other investigational trials within 30 days; or patients with any other medical condition that, in the opinion of the investigators, could make the patient inappropriate for this study were excluded.
Research methods
All selected patients were randomly divided into an experimental group and a control group through a computer-generated randomization sequence. Warfarin was administered with different initial doses among the patients from the experimental group and the control group, and the target INR values were within the therapeutic range of 1.8-3.0.
In the experimental group, the polymorphisms of CYP2C9 and VKORC1 were detected to identify VKORC1 and CYP2C9 genotypes and then to calculate the warfarin dose (“predicted dose”) before the scheduled surgery. Patients were administered oral warfarin at the dosage of the “predicted dose” beginning 3 days following surgery. As patients are more sensitive to warfarin immediately after surgery, the highest initial warfarin dose was not higher than 3.5mg/day, even if the “predicted dose” was more than that. After 3 days of anticoagulant therapy, warfarin doses were adjusted depending on the measured INR values. In the control group, warfarin was initiated at 2.5 mg/day, which is currently the standard initiation dose in China, and it was adjusted based on the INR values.
With reference to the literature [5], “predicted dose (mg/d) ” = exp [0.727- 0.007 × age (years) + 0.384 × Body surface area (m2) + 0.403×VKORC1 6484TC + 0.554 × VKORC1 6484CC - 0.482×CYP2C9*1/*3 - 1.583 × CYP2C9*3/*3]. (BSA (m2) = 0.0061 × height (cm) + 0.0128 × weight (kg) - 0.1529, VKORC1 6484TC, VKORC1-6484CC, CYP2C9*1/*3, CYP2C9 *3/*3 yes or no was taken as 1 or 0, respectively; exp referred to the exponent of natural logarithm).
All patients were followed up for 50 days after initiation of warfarin therapy, to compare the outcomes between the experimental group and the control group. Patients' INR was measured daily after their operations during hospitalization and twice a week after they discharged from the hospital. Stable warfarin maintenance dose was defined as the dose that led to the patient's INR values within the therapeutic range of 1.8-3.0 measured at least 7 days [6]. The adverse outcomes included INR greater than 3.5, bleeding, or venous thrombosis after warfarin therapy. The primary endpoint was the time to reach a stable warfarin maintenance dose. The secondary endpoints were time within therapeutic INR range; time of dose adjustment in hospital; the proportion of patients who obtained stable dose; and incidence of adverse outcome.
Polymorphisms of CYP2C9 and VKORC1
The polymorphisms of CYP2C9 and VKORC1 were detected by using PCR-RFLP method. A blood sample (2.0ml, citrated) was drawn 24 hours before the scheduled surgery and was coagulated. The genome DNA was extracted by using DNA extraction kit methods (Tiangen Biological Technology Limited Company) and then was frozen at -20℃ until analysis. With reference to the literature [7], according two single nucleotide polymorphisms (SNP) sites of VKORC1 1173C>T and CYP2C9 1075A>C genes, three premiers were designed respectively: two of them was forward primers whose 3-end matched the wild type and mutants bases in the two SNP sites, respectively, and whose 5-end were introduced “GC” sequences, and one of them was a reverse primer (as shown in Table 1). The genotype frequency of CYP2C9 430C>T was uncommon in Han population and identification absent in this study. The primers were from Biomedical Engineering Co., Ltd, Shanghai, and SYBR GreenⅠfluorescent dye from Baiweixin Corp, Xiamen.
PCR primer.
| SNP sites | Premier (5'→3') | Length (bp) | Tm (℃) |
|---|---|---|---|
| VKORC1 | FT:GCCGAGGAGGAGCCGAGGGAGCGAGCCGCCAGGAGATCATCGAgT | 90 | 86.9 |
| 1173C>T | FC:GCCAGGAGATCATCGAaC | 63 | 84.1 |
| R:CACCTGGGCTATCCTCTG | |||
| CYP2C9 | FA:GGGAGCCCGACCACGGACGGAGGCACCGCACGAGGTCCAGAGATACA | 117 | 84.1 |
| 1075A>C | FC:CACGAGGTCCAGAGATACC | 89 | 82 |
| R:GGAATGAGATAGTTTCTGAATTTAAT |
F, forward primer; R, reverse primer; Tm, melting temperature.
The PCR products were analyzed by the melting curve (ABI-7500 fluorescence quantitative PCR) to identify the genotype. The melting curve of VKORC1 1173TT and CYP2C9*1/*1 showed a single-peak curve at the higher melting temperature, the melting curve of VKORC1 1173CC and CYP2C9*3/*3 showed a single-peak curve at the lower melting temperature, and the melting curve of VKORC1 1173TC and CYP2C9*1/*3 showed a double-peak curve at the higher and the lower melting temperature.
Statistical Analysis
The sample size calculations are based on an estimated receiving warfarin maintenance dose during 50-day of follow-up of 85% for administration of warfarin according to pharmacogenetic-based warfarin-dosing algorithm and 60% for conventional administration of warfarin. With an α level of 0.05 and a test power of 0.80, the resulting sample size was 46 patients for each group. A risk of loss of patients to follow up of 1-5% was assumed.
Statistical analysis was performed using the SPSS 13.0 statistical software package. All p values less than 0.05 were considered to be statistically significant. The unpaired t test or t' test according to the homogeneity test for variance was used to compare measurement data and Fisher's exact test was used to compare enumeration data. The time elapse from initiation of warfarin therapy until warfarin maintenance dose was analyzed with the Kaplan-Meier method and compared with the Log-rank test. The hazard ratio and its confidence intervals (CI) were estimated using the Cox regression model. Time elapse was analyzed from initiation of warfarin therapy until warfarin maintenance dose using Cox proportional hazards regression to control for potentially confounding factors. The differences between predicted dose and actual dose were analyzed with the paired-samples t-test, and the linear correlation between them was analyzed using the correlation analysis.
Results
Study population
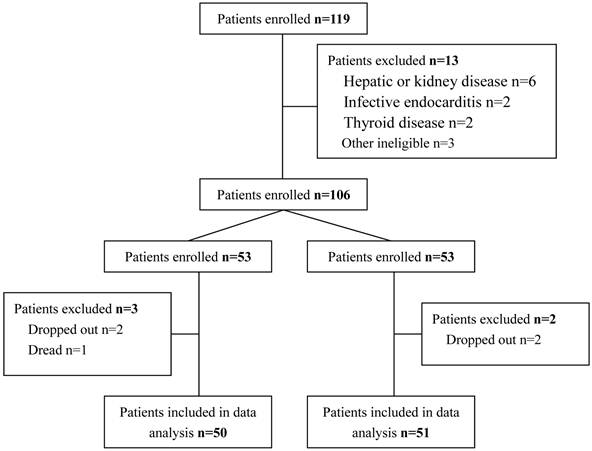
From January 2010 to June 2010, a total of 119 consecutive patients of Han nationality (38 male and 81 female, with an average age of 42.3 ±7.1 years old) with rheumatic heart disease met the inclusion criteria. Thirteen patients were excluded because of liver disease (4 cases), kidney disease (2 cases), infective endocarditis (2 cases), thyroid disease (2 cases), or requiring use of other drugs known to be related to CYP2C9 and VKORC1 (3 cases), and then 106 patients were followed into this study and randomly divided into an experimental group (n=53) and a control group (n=53). During 50-day of follow-up, an additional 5 patients were excluded from further analysis for the following reasons: two patients in the experimental group and two in the control group dropped out during follow-up, and one patient in the experimental group died of postoperative complications that were not related to warfarin therapy. Therefore, the outcome analysis was conducted on 50 patients in the experimental group and 51 patients in the control group (Figure 1).
Flow of the patients enrolled in the study.
Sixty-nine underwent single mechanical prosthetic valve replacement (4 patients with concomitant coronary artery disease underwent simultaneous coronary artery bypass grafting), and 32 double mechanical prosthetic valve replacement (2 patients with concomitant coronary artery disease underwent simultaneous coronary artery bypass grafting). Among patients undergoing simultaneous coronary artery bypass grafting, 4 patients received one bypass conduit (great saphenous vein graft was used as bypass conduit in 3 patients, and left internal mammary artery in 1 patient), and 2 patients two bypass conduits (sequential great saphenous vein graft was used as bypass conduit in 2 patients).
The characteristics of the entire cohort were shown in Table 2. There were no significant differences in age, gender, body surface area, operation, left ventricular ejection fraction, left atrial size, and basal INR as well as cardiac rhythm between groups. No differences were observed in the distribution frequency of VKORC1 genotype and CYP2C9 genotype between two groups.
Characteristics of the entire cohort
| Experimental Group (n=50) | Control Group (n=51) | p | |
|---|---|---|---|
| Age (years old) | 41.9±6.3 | 42.8±8.5 | 0.548 |
| Gender (male/female) | 15/35 | 16/35 | 1.000 |
| Height (cm) | 160.3±5.8 | 160.1±7.2 | 0.878 |
| Weight (kg) | 51.7±7.5 | 52.2±8.5 | 0.755 |
| BSA (m2) | 1.57±0.14 | 1.59±0.16 | 0.506 |
| Basal INR | 0.94±0.11 | 0.91±0.09 | 0.136 |
| Baseline cardiac rhythm | 0.315 | ||
| Atrial fibrillation | 18 (36.0%) | 24(47.1%) | |
| Sinus rhythm | 32 (64.0%) | 27 (52.9%) | |
| Concomitant CAD | 2 (4.0%) | 4 (7.8%) | 0.678 |
| Ejection fraction (%) | 55.5±7.4 | 57.3±6.5 | 0.197 |
| Left atrial size (mm) | 51.6±6.3 | 50.3±7.2 | 0.337 |
| Operation | 0.831 | ||
| Single VR with/without CABG | 35 | 34 | |
| Double VR with/without CABG | 15 | 17 | |
| VKORC1(TT:TC:CC) | 44:6:0 | 41:9:1 | 0.528 |
| CYP2C9(*1/*1:*1/*3:*3/*3) | 48:2:0 | 49:2:0 | 0.951 |
BSA, body surface area; INR, international normalized ratio; CAD, coronary artery disease; VR, valve replacement.
Polymorphisms of CYP2C9 and VKORC1
Different VKORC1 1173C>T genotypes and CYP2C9 1075A>C genotypes had different peak melting curves. For VKORC1 1173C>T, the amplification segment of allele T had high melting temperature compared to allele C (82.14 ± 0.10 ℃ versus 77.10 ± 0.15 ℃). So, the melting curve of homozygous TT and CC respectively showed a single-peak curve at 82.14 ℃ and at 77.10 ℃, and the melting curve of heterozygous TC showed a double-peak curve at 82.14 ℃ and 77.10 ℃. Similarly, for CYP2C9 1075A>C, the amplification segment of allele A (CYP2C9*1) had high melting temperature compared to allele C (CYP2C9*3) (86.16 ± 0.08 ℃ versus 81.85 ± 0.12 ℃). The melting curve of homozygous AA (CYP2C9*1/*1) showed a single-peak curve at 86.16 ℃, the melting curve of homozygous CC (CYP2C9*3/*3) showed a single-peak curve at 81.85 ℃, and the melting curve of heterozygous AC (CYP2C9*1/*3) showed a double-peak curve at 81.85 ℃ and 86.16 ℃. The average melting temperature of the amplification segments of different alleles came from 134 normal controls.
Clinical application
In this study, a total of 72 patients reached stable warfarin maintenance dose during 50-day of follow-up. Compared to the control group, patients in the experimental group had shorter time elapse from initiation of warfarin therapy until stable warfarin maintenance dose (mean time: 27.5 ± 1.8 d versus 34.7 ± 1.8 d, p<0.001; median time: 24.0 ± 1.7 d versus 33.0 ± 4.5 d, p<0.001).
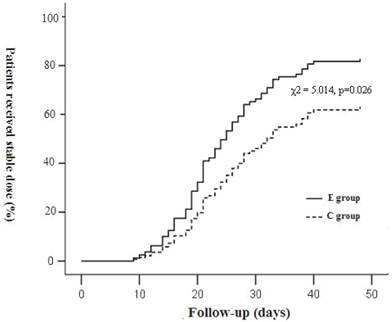
Four factors (group, gender, age, BSA) were entered into Cox proportional hazards regression. Cox regression revealed that group and age were two significant variables related to the time elapse from initiation of warfarin therapy until stable warfarin maintenance dose. After the Cox proportional model was used, the hazard ratio for group (experimental versus control group) was 1.568 (95%CI 1.103-3.284; p=0.026) (as shown in Figure 2). During 50-day of follow-up, 84.0% patients (42/50) in the experimental group and 58.8% patients (30/51) in the control group received warfarin maintenance dose (p=0.0078). In addition, Cox regression also showed the older the age, the longer the time elapse from initiation of warfarin therapy until stable warfarin maintenance dose. As shown in Table 3, the median time elapse from initiation of warfarin therapy until stable warfarin maintenance dose was 21 days for patients below 30 years old, 25 days for 30-39 years old, 28 days for 40-49 years old, and 37 days for over 50 years old, respectively (χ2=9.199, p=0.027).
Patients received stable warfarin maintenance dose during follow-up. E group: the experimental group; C group, the control group.
Effect of age on time elapse from initiation until stable warfarin maintenance dose.
| Age (years) | Average time(days) | Median time(days) | χ2 | p |
|---|---|---|---|---|
| <30 (n=10) | 26.2±2.2 | 21.0±2.3 | 9.199 | 0.027 |
| 30~39 (n=11) | 28.5±3.4 | 25.0±2.2 | ||
| 40~49 (n=26) | 31.7±2.3 | 28.0±2.3 | ||
| ≥50 (n=25) | 37.2±1.7 | 37.0±3.4 |
Five patients (10.0%) in the experimental group and eight patients (15.7%) in the control group suffered adverse events (either hemorrhage or INR over 3.5) during 50-day of follow-up (p=0.55). Compared to the control group, patients in the experimental group had longer time elapse from initiation of warfarin therapy until adverse events (45.2 ± 3.5 d versus 42.7±2.4 d), but no significant difference was found (p=0.15).
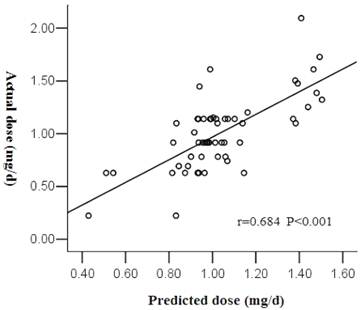
Forty-two patients in the experimental group, who received stable warfarin maintenance dose during 50-day of follow-up, had higher predicted dose compared to the actual dose (2.87±0.67 mg/d versus 2.81±0.78 mg/d), but no significant difference was found through the paired-samples t-test (t=0.38, p=0.71). As shown in Figure 3, the predicted dose was prominently correlative with the actual dose through the correlation analysis (r=0.684, p<0.001).
Correlation between predicted dose and actual dose.
Discussion
Genetic factors, such as the polymorphisms of VKORC1 and CYP2C9, played increasingly important roles in the inter-individual variability in warfarin dose [8-10]. Previous studies [1-4] concentrated mainly on establishing genetic-based warfarin-dosing algorithm, with few researches focusing on verifying these algorithms and evaluating these clinical values through randomized and controlled trials. This randomized and controlled trial aimed to evaluate the feasibility of clinical application of the pharmacogenetic-based warfarin-dosing algorithm (based on CYP2C9 and VKORC1 genotypes) to predict warfarin maintenance dose in patients of Han nationality with rheumatic heart disease undergoing valve replacement. In this study, patients in the experimental group had shorter time elapse from initiation of warfarin therapy until stable warfarin maintenance dose compared to the control group (mean time: 27.5 ± 1.8 d versus 34.7 ± 1.8 d, p<0.001; median time: 24.0 ± 1.7 d versus 33.0 ± 4.5 d, p<0.001), indicating that pharmacogenetic-based warfarin-dosing algorithm (based on CYP2C9 and VKORC1 genotypes) may effectively shorten the time elapse from initiation of warfarin therapy until stable warfarin maintenance dose, which was consistent with the results of two randomized and controlled studies in the white race [11, 12]. A Taiwan population-based study by Wen [13] showed that 83% patients who were orally administrated with warfarin based on predicted dosing algorithm received stable warfarin maintenance dose within 2 weeks, and it leg to the conclusion that genetic-based predicted dosing algorithm was conducive to reduce the time elapse from initiation of warfarin therapy until stable warfarin maintenance dose. The conclusion draw by Wen, however, failed in persuasiveness because no control group was designed in the Taiwan population-based study. In this study, Cox proportional hazards regression revealed that group and age were two significant variables related to the time elapse from initiation of warfarin therapy until stable warfarin maintenance dose. Through Cox proportional model, the hazard ratio for group (experimental versus control group) was 1.568 (95%CI 1.103-3.284; p=0.026), which meant during the same follow-up period and at the same sample size, the number of patients in the experimental group receiving stable warfarin maintenance dose was 1.568 times higher than that in the control group. In this study, 84.0% patients in the experimental group and 58.8% patients in the control group received warfarin maintenance dose during 50-day of follow-up (p=0.0078), which corresponded with the result of the Cox proportional model mentioned above. This study also displayed that age was not only a factor related to the inter-individual variability in warfarin dose, but also one of main factors related to the time elapse from initiation of warfarin therapy until stable warfarin maintenance dose, which was scarcely reported in previous studies. In this study, patients over 50 years old had longer time elapse from initiation of warfarin therapy until stable warfarin maintenance dose, compared with patients below 50 years old. The older the age, the longer the time elapse from initiation of warfarin therapy until stable warfarin maintenance dose, which possibly caused by compensatory dysfunction of organs in older patients.
In this study, 84% patients in the experimental group received warfarin maintenance dose during 50-day of follow-up, and the predicted dose was prominently correlated with the actual one through the correlation analysis (r=0.684, p<0.001), indicating that our pharmacogenetic-based warfarin-dosing algorithm could effectively predict the actual warfarin maintenance dose. Based on a combination of genetic factors and non-genetic factors, the predicted algorithm of warfarin maintenance dose had a strong predicted efficacy, could effectively shorten the time elapse from initiation of warfarin therapy until stable warfarin maintenance dose, and was proved a feasible clinical application.
In this study, 10.0% patients in the experimental group and 15.7% patients in the control group suffered adverse events (either hemorrhage or INR over 3.5) during 50-day of follow-up (p=0.55). And patients in the experimental group had long time elapse from initiation of warfarin therapy until adverse events, compared to the control group (45.2 ± 3.5 d versus 42.7 ± 2.4 d, p=0.15). It remains to be clarified by increasing the sample size whether the predicted algorithm of warfarin maintenance dose reduced effectively the incidence of adverse events.
In addition, 42 patients in the experimental group, who received stable warfarin maintenance dose during 50-day of follow-up, had higher predicted dose compared to the actual dose (2.87±0.67 mg/d versus 2.81±0.78 mg/d, p=0.71). The difference between the predicted dose and the actual one may be due to other genes related with the pharmacology of warfarin not involved in our predicted algorithm of warfarin maintenance dose. And, non-genetic factors, such as eating habits, concomitant with other drugs, and individual differences in the patients' condition, may result in the difference between predicted dose and the actual one. With more pharmacological effects of warfarin-related genes clarified, and more non-genetic factors involved, the predicted algorithm of warfarin maintenance dose would be more accurate, contributing to the clinical application of individualized warfarin, improving the effectiveness and safety of warfarin.
In conclusion, based on CYP2C9 and VKORC1 genotypes, the pharmacogenetic-based warfarin-dosing algorithm may shorten the time elapse from initiation of warfarin therapy until warfarin maintenance dose. It is feasible for the clinical application of the pharmacogenetic-based warfarin-dosing algorithm in patients of Han nationality with rheumatic heart disease after valve replacement. It, however, needs further study whether or not our predicted algorithm of warfarin maintenance dose was applicable to patients of other nationality in the country.
Competing Interests
The authors have declared that no competing interest exists.
References
1. Wadelius M, Chen LY, Eriksson N. et al. Association of warfarin dose with genes involved in its action and metabolism. Hum Genet. 2007;21:23-34
2. Yin T, Miyata T. Warfarin dose and the pharmacogenomics of CYP2C9 and VKORC1 - rationale and perspectives. Thromb Res. 2007;120:1-10
3. Bodin L, Verstuyft C, Tregouet DA. et al. Cytochrome P450 2C9 (CYP2C9) and vitamin K epoxide reductase (VKORC1) genotypes as determinants of acenocoumarol sensitivity. Blood. 2005;106:135-140
4. D'Andrea G, D'Ambrosio RL, Di Perna P. et al. A polymorphism in the VKORC1 gene is associated with an interindividual variability in the dose-anticoagulant effect of warfarin. Blood. 2005;105:645-649
5. Huang SW, Chen HS, Wang XQ. et al. Validation of VKORC1 and CYP2C9 genotypes on interindividual warfarin maintenance dose: a prospective study in Chinese patients. Pharmacogenet Genomics. 2009;19:226-234
6. Voora D, Eby C, Linder MW. et al. Prospective dosing of warfarin based on cytochrome P-450 2C9 genotype. Thromb Haemost. 2005;93:700-705
7. Huang SW, Li Q, Zhu SY, Li L, Xiong F, Jia YK, Xu XM. SYBR Green-based real-time PCR assay for detection of VKORC1 and CYP2C9 polymorphisms that modulate warfarin dose requirement. Clin Chem Lab Med. 2009;47:26-31
8. Veenstra DL, You JH, Rieder MJ. et al. Association of Vitamin K epoxide reductase complex 1 (VKORC1) variants with warfarin dose in a Hong Kong Chinese patient population. Pharmacogenet Genomics. 2005;15:687-691
9. Aquilante CL, Langaee TY, Lopez LM. et al. Influence of coagulation factor, vitamin K epoxide reductase complex subunit 1, and cytochrome P450 2C9 gene polymorphisms on warfarin dose requirements. Clin Pharmacol Ther. 2006;79:291-302
10. Lee SC, Ng SS, Oldenburg J. et al. Interethnic variability of warfarin maintenance requirement is explained by VKORC1 genotype in an Asian population. Clin Pharmacol Ther. 2006;79:197-205
11. Caraco Y, Blotnick S, Muszkat M. CYP2C9 genotype-guided warfarin prescribing enhances the efficacy and safety of anticoagulation: a prospective randomized controlled study. Clin Pharmacol Ther. 2008;83:460-470
12. Anderson JL, Horne BD, Stevens SM. et al. Randomized trial of genotype-guided versus standard warfarin dosing in patients initiating oral anticoagulation. Circulation. 2007;116:2563-2570
13. Wen MS, Lee M, Chen JJ. et al. Prospective study of warfarin dosage requirements based on CYP2C9 and VKORC1 genotypes. Clin Pharmacol Ther. 2008;84:83-89
Author contact
![]() Corresponding author: Prof. ShiTao Cui, bojidefeiyingcom, or Prof. Ke Fei, drfeikecom.cn; Dr. Qiang Ji, drjiqiangedu.cn.
Corresponding author: Prof. ShiTao Cui, bojidefeiyingcom, or Prof. Ke Fei, drfeikecom.cn; Dr. Qiang Ji, drjiqiangedu.cn.