Impact Factor ISSN: 1449-1907

 Global reach, higher impact
Global reach, higher impactInt J Med Sci 2011; 8(7):529-536. doi:10.7150/ijms.8.529 This issue Cite
Research Paper
The Clinical Significance of Digital Examination-Indicated Cerclage in Women with a Dilated Cervix at 14 0/7 - 29 6/7 Weeks
Hyun Sun Ko1, Yun Seong Jo1, Ki Cheol Kil1, Ha Kyun Chang1, Yong-Gyu Park2, In Yang Park1, Guisera Lee1, Sajin Kim1, Jong Chul Shin1 ![]()
1. Department of Obstetrics and Gynecology, College of Medicine, Catholic University, Seoul, Korea;
2. Department of Biostatistics, College of Medicine, Catholic University of Korea
Received 2011-7-2; Accepted 2011-8-29; Published 2011-9-6
Abstract
Objective. This study was to compare pregnancy outcomes between cerclage and expectant management in wemen with a dilated cervix. Design. Retrospective multicenter cohort study. Setting. Five hospitals of Catholic University Medical Center Network in Korea. Population. A total of 173 women between 14 0/7 and 29 6/7 weeks' gestation with cervical dilation of 1 cm or greater by digital examination. Methods. Pregnancy outcomes were compared according to cerclage or expectant management, with the use of propensity-score matching. Main Outcome Measures. Primary outcome was time from presentation until delivery (weeks). Secondary outcomes were gestational age at delivery, neonatal survival, morbidity, preterm birth, and so on.
Results. Of 173 women, 116 received a cerclage (cerclage group), and 57 were managed expectantly without cerclage (expectant group). Cervical dilation at presentation, and the use of amniocentesis performed to exclude subclinical chorioamnionitis differed between two groups. In the overall matched cohort, there was significant difference in the time from presentation until delivery (cerclage vs. expectant group, 10.6±6.2 vs. 2.9±3.2 weeks, p <0.0001). While there was no significant difference in the neonatal survival between two groups, there werelower neonatal morbidity as well as higher pregnancy maintenance rate at 28, 32, 34 and 37 weeks' gestation in the cerclage group, compared with the expectant group.
Conclusion. This study suggests that digital examination-indicated cerclage appears to prolong gestation and decrease neonatal morbidity, compared with expectant management in women with cervical dilation between 14 0/7 and 29 6/7 weeks.
Keywords: Cerclage, Cervical dilation, Preterm birth
Introduction
Preterm birth and its consequences constitute a major health problem in the worldwide. Many preventative strategies have been tried, including progesterone supplementation, antibiotic usage, tocolytics and cervical cerclage, but the incidence has not reduced (1).
Physical or digital examination-indicated cerclage, defined as a cerclage placed because of cervical dilation, regardless of cervical length, obstetric history, or risk factors for preterm birth, has been suggested as a therapy for these women. There is no intervention proven to prevent preterm birth in women with second-trimester cervical dilation. Indomethacin therapy in women with dilated cervix at 14 0/7 to 25 6/7 weeks, regardless of cerclage or not, had no effect on pregnancy outcomes (2). Cerclage in women with cervical dilation has been studied in only one randomized trial of 23 women, including both singleton and twin gestations (3). Women with cervical dilation at preterm have been shown to have high rates of inflammation and possibly of contractions. Recently, one large cohort study reported that physical examination-indicated cerclage appears to prolong gestation and improve neonatal survival, compared with expectant management in selected women with cervical dilation between 14 0/7 and 25 6/7 weeks (4).
It has been demonstrated that the rates of neonatal mortality and complications are significant in preterm babies born prior to 32 weeks of gestation and with body weight less than 1,500 g (5,6). The incidence of perinatal death has been considerably decreased as the neonatology has been making its advance, but it is still a critical issue to manage morbidity and mortality after preterm delivery. Gestational age can be one of the most important predictors of morbidity and mortality of neonates. Whereas the group of infants with the greatest risk of morbidity and mortality comprises those born at less than 32 weeks of gestation, infants born between 32 and 36 weeks represent the greatest number of infants born preterm (7). The latter group of infants also experiences a greater risk for health and developmental problems compared with the risk for infants born at term(7). It is clear that the rates of infant survival and of being born as normal infants are high as gestational age approaches close to the full term. There is need to investigate the value of cerclage including the women with cervical dilation between 26 0/7 and 29 6/7 weeks.
The objectives of our study was to estimate fetal and maternal outcomes associated with physical examination-indicated cerclage, compared with expectant management in women with cervical dilation between 14 0/7 and 29 6/7 weeks' gestation.
Methods
This is a retrospective cohort study of the women with cervical dilation between 14 0/7 and 29 6/7 weeks' gestation who received expectant management or digital-examination indicated cerclage, between January 2000 and June 2010 at 5 centers in Catholic University Medical Center of Korea. Approval by the institutional review board was obtained at each participating center. Participating centers were all university teaching or tertiary care centers with neonatal intensive care units with the ability to administer surfactant and vasopressors and provide ventilator support to neonates. Primary outcome was time from presentation until delivery (weeks). Secondary outcomes were gestational age at delivery, neonatal survival, significant neonatal morbidity, preterm birth less than 28, 32, 34, 37 weeks, and birth weight less than 1500g. Significant neonatal morbidity included respiratory distress syndrome requiring surfactant, sepsis, intracranial hemorrhage, necrotizing enterocolitis, and bronchopulmonary dysplasia.
Inclusion criteria
The women followed up in this study were initially identified in 1 of 2 ways: 1) those found to have a shortened cervix or suspected cervical dilation on ultrasound or 2) those identified by digital examination performed because of a history of prior second trimester loss, history of preterm birth, or subjective complaints of pressure or discharge. The subjects with cervical dilatation of 1 cm or greater by digital examination between 14 0/7 and 29 6/7 weeks' gestation were included.
Exclusion criteria
Subjects with preterm premature rupture of membranes (PPROM), active labor, vaginal bleeding, or chorioamnionitis at time of presentation and those with a closed cervix on digital examination were excluded. PPROM was defined by gross rupture of amniotic fluid with oligohydramnios or anhydramnios on ultrasound, or visualizing amniotic fluid collection on sterile speculum exam, with the presence of a Nitrazine positive vaginal pool of fluid. Active labor was defined as the presence of regular uterine contractions 3 or more in 10 minutes with cervical change. Chorioamnionitis was defined by the following: 1) positive amniotic fluid culture (aerobic and anaerobic bacteria, ureaplasma, or mycoplasma); 2) the combination of positive amniotic fluid Gram stain, amniotic fluid leukocyte count greater than 50 cells/mm3, and/or amniotic fluid glucose 14 mg/dL or less; 3) interleukin-6 greater than 2 ng/mL at centers at which this test was available; or 4) clinical chorioamnionitis as defined by Gibbs et al (8).
Subjects were not randomly assigned to a particular management strategy. Clinical management was made case by case between the physician and patient after an informed discussion. Physical examination-indicated cerclage was available at all centers participating in this study.
Mcdonald Cerclage was performed under spinal anesthetic in a 'head down' position, using a Mersilene tape (Ethicon, Inc, Somerville, NJ). A Foley catheter or sponge forceps was used to replace the membranes through the cervix if the membrane is protruded through the cervical canal or visible beyond the external orifice of the uterus. Management thereafter involved bed rest or nifedipine or sympathomimetics, antibiotics on an individual basis. The sutures were removed in all women who labored, ruptured their membranes and developed clear evidence of infection or on reaching 37 weeks' gestation.
After application of the inclusion and exclusion criteria as described, 173 women of the 308 women with dilated cervix were included in this investigation. Thereof 116 received operative (Cerclage group) and 57 expectant treatment (Expectant group).
Statistical Analysis
For observed cohort data, comparison of categorical variables was used by χ2 test, whereas independent t-test was used to compare continuous variables.
To reduce the effect of treatment-selection bias and potential confounding in this observational study, we performed rigorous adjustment for significant differences in the prognostic factors such as gestational age at diagnosis, cervical dilation at diagnosis, previous cervical incompetence, and amniocentesis performed to exclude subclinical chorioamnionitis which were significantly or marginally significantly different between two groups with the use of propensity-score matching (9, 10).
After all the propensity-score matches were performed, we compared the baseline covariates between two groups. Continuous variables were compared with the use of the mixed model analysis and categorical variables were compared with the use of Generalized estimating equations (GEE) analysis. GEE analysis was also used to obtain the matched odds ratio and its 95% confidence interval.
Survival curves were obtained by Kaplan-Meier estimates and compared by of Cox regression models with robust standard errors that accounted for the clustering of matched pairs (11, 12).
All reported p values are two-sided, and p values of less than 0.05 were considered to indicate statistical significance. SAS software, version 9.1was used for statistical analyses.
Details of ethics approval
Ethical approval was granted by the Catholic Medical Center, Central Ethics Board (XC11RIMI0002K) at Jan 14, 2011.
Results
A total of 308 women between 14 0/7 and 29 6/7 weeks' gestation with suspected cervical dilation 1 cm or greater were identified, during the study perioid. Of these 308 women, 7 were excluded because of cervical dilation less than 1 cm. An additional 69 were found to have contraindications to cerclage (Figure 1). Of the 232 remaining subjects, 6 wanted for induction of labor or surgical termination.
Flow diagram of all identified women between 14 0/7-29 6/7 weeks
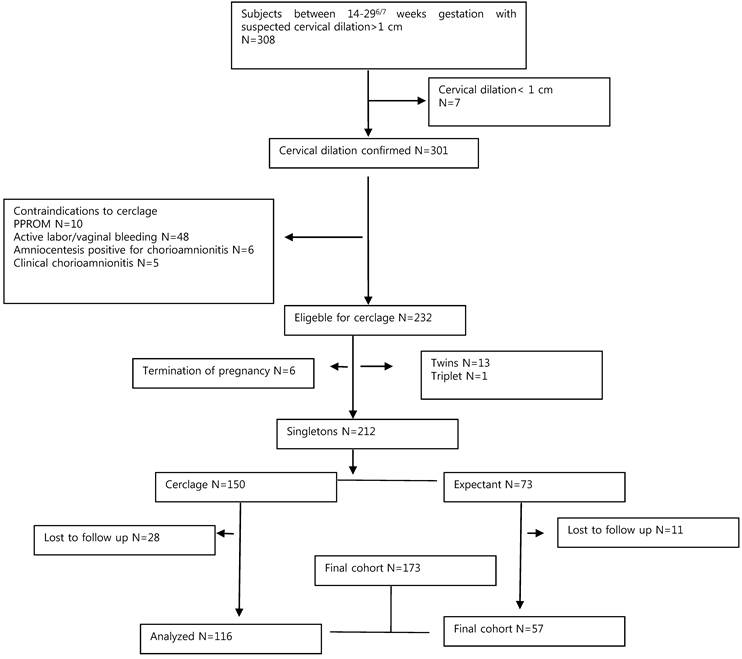
These patients were followed up for the development of any maternal complications but were excluded from this analysis. Women with multifetal gestations were excluded (13 twins, 1 triplet), and of the remaining 212 singletons, outcomes were available in 81.6% (28 women in the cerclage group and 11 women in the expectant group were lost to follow-up), leaving 173 women in the final cohort. Statistical analysis was conducted on these 173 women, 57 who were managed without cerclage and 116 who underwent cerclage placement at the obstetrician's discretion.
There were no statistical difference in mean ages, parities, and gestational age at presentation with similar rates of prior preterm birth and abortion, between cerclage group and expectant group (Table 1). Although women receiving cerclage seemed more likely to have had a previous second-trimester miscarriage, there was no statistical difference. Mean cervical dilation of subjects undergoing cerclage was less than in expectant group (p < 0.0001); however, the use of amniocentsis performed to exclude subclinical chorioamnionitis was lower in the group receiving cerclage (p=0.0293). Gestational weeks at diagnosis and history of previous cervical incompetence were marginally significantly different between two groups (p=0.051 and p=0.0555, respectively). The incidence of antenatal steroid administration did not differ.
Baseline Characteristics of the observed cohort
| Cerclage group (N=116) | Expectant group (N=57) | P-value | |
|---|---|---|---|
| Age* | 31.42±3.82 | 30.86±4.79 | 0.4409 |
| Parity* | 0.99±1.04 | 0.98±0.88 | 0.9557 |
| Previous preterm birth* | 0.32±0.49 | 0.39±0.56 | 0.419 |
| Previous abortion* | 0.78±1.03 | 1.07±1.57 | 0.2095 |
| Gestational week at diagnosis* | 22.42±4.14 | 23.51±3.04 | 0.051 |
| Cervical dilatation at diagnosis* | 1.99±1.22 | 3.35±1.71 | <0.0001 |
| Previous cervical incompetence* | 0.16±0.45 | 0.3±0.50 | 0.0555 |
| Amniocentesis performed to exclude subclinical chorioamnionitis** | 27(23.3) | 22(39.3) | 0.0293 |
| Antenatal steroids administered** | 46(39.7) | 25(44.7) | 0.5336 |
| Gestational week at delivery* | 33.12±5.80 | 25.47±4.76 | <0.0001 |
* independent t test ** Chi-square test
Values are expressed as mean±SD or n (%).
Characteristics of Patients Matched for Propensity Scores
After propensity-score matching was performed for the entire population, there were 20 (2:1) matched pairs of 40 patients who received cerclage and 20 patients who received conservative care.
In the matched cohorts, there was no longer any significant difference between the cerclage group and the expectant group for any covariate, especially, gestational week and cervical dilation at diagnosis, history of previous cervical incompetence, and the use of amniocentesis performed to exclude subclinical chorioamnionitis, which were significantly or marginally significantly different before propensity score matching (Table 2).
Baseline Characteristics of the Propensity-Matched Patients
| Cerclage group (N=40) | Expectant group (N=20) | P-value | |
|---|---|---|---|
| Age* | 31.95±4.33 | 32.25±5.26 | 0.8067 |
| Parity* | 1.00±0.96 | 0.90±0.97 | 0.7285 |
| Previous preterm birth* | 0.33±0.47 | 0.30±0.57 | 0.8578 |
| Previous abortion* | 0.62±0.85 | 0.95±1.03 | 0.1404 |
| Gestational week at diagnosis* | 23.05±3.95 | 24.29±2.59 | 0.1296 |
| Cervical dilatation at diagnosis* | 1.83±0.87 | 1.75±0.79 | 0.4982 |
| Previous cervical incompetence* | 0.13±0.33 | 0.05±0.22 | 0.3492 |
| Amniocentesis performed to exclude subclinical chorioamnionitis** | 6(15.0) | 3(15.0) | 1.0000 |
| Antenatal steroids administered** | 19(47.5) | 14(70.0) | 0.1282 |
* Mixed model analysis ** GEE analysis
Values are expressed as mean±SD or n (%).
Outcomes for the Matched Cohort
Table 3 shows the clinical outcomes according to the treatment approach in the overall matched cohort. The analysis of the primary outcome showed a significant increase in pregnancy prolongation (mean 10.6 vs. 2.9 weeks, P < 0.0001) and gestational age at delivery (mean 33.7 vs. 27.2 weeks, P < 0.0001) in the cerclage group, compared with the expectant group.
Pregancy outcomes of the Propensity-Matched Patients.
| Cerclage group (N=40) | Expectant group (N=20) | P-value | |
|---|---|---|---|
| Interval from presentation to delivery (weeks) * | 10.64±6.22 | 2.94±3.21 | <0.0001 |
| Gestational week at delivery* | 33.70±5.35 | 27.23±4.42 | <0.0001 |
| Birth weight (g) * | 2203±987.69 | 1112±611.87 | <0.0001 |
| Apgar score at 1 minute* | 6.13±2.85 | 3.35±2.58 | 0.0012 |
| Apgar score at 5 minutes* | 7.23±3.05 | 4.55±3.07 | 0.0049 |
| Preterm birth less than 28 weeks** | 8(20.0) | 13(65.0) | <0.0001 |
| Preterm birth less than 32 weeks** | 14(35.0) | 17(85.0) | 0.0018 |
| Preterm birth less than 34 weeks** | 19(47.5) | 19(95.0) | 0.0046 |
| Preterm birth less than 37 weeks** | 26(65.0) | 20(100.0) | <0.0001 |
| Birthweight less than 1500g** | 10(25.0) | 15(75.0) | 0.0002 |
| Birthweight less than 2000g** | 19(47.5) | 18(90.0) | 0.004 |
| Neonatal survival** | 34(85.0) | 12(60.0) | 0.0923 |
| Significant neonatal morbidity** | 15(37.5) | 16(80.0) | 0.0036 |
* Mixed model analysis ** GEE analysis
Values are expressed as mean±SD or n (%).
Significant neonatal morbidity: respiratory distress syndrome which needs administration of surfactant, sepsis, intracranial hemorrhage, necrotizing enterocolities, and bronchopulmonary dysplasia.
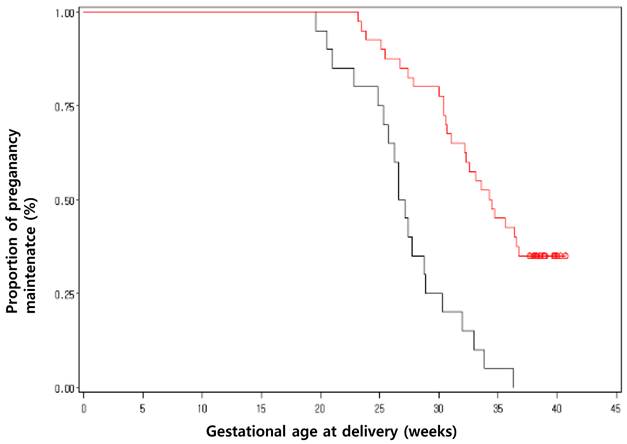
Birth weight, Apgar score, preterm birth at less than 28, 32, 34, and 37 weeks, and birth weight less than 1500 and 2000g were all improved by clinically-indicated cerclage. 65% (13 of 20) of women who were expectantly managed delivered prior to 28 weeks, compared with 20% (8 of 40) of women who received a cerclage. Also, 95% (19 of 20) and 100% (20 of 20) of women who were expectantly managed delivered prior to 34 weeks and 37 weeks, compared with 47.5% (19 of 40) and 65% (26 of 40) women who received a cerclage (Table 3 and Figure 2). While the analysis for the neonatal survival failed to demonstrate a difference (85.0% vs. 60.0%, P=0.0923), it demonstrated a difference in the rate of significant neonatal morbidity (37.5% vs. 80.0%, P=0.0036) between the cerclage and expectant groups. The proportion of pregnancy maintenance until 37 weeks was significantly higher in cerclage group (p< 0.001) (Figure 2).
Kaplan-Meier curves for pregnancy maintenance in propensity matched patients who underwent cerclage or expectant management. Propensity matching for the entire cohort created 20 (2:1) matched pairs of patients. Survival curves show the gestational weeks without delivery following cerclage or expectant management (p < 0.001).
Significant neonatal morbidity decreased to 0.15 fold in the cerclage group, compared to the expectant group. The use of digital examination-indicated cerclage was associated with a greater than 3-, 10-, and 21-fold increase in birth after 28, 32, and 34 weeks, respectively, as well as 9- and 10-fold increase in birth weight greater than 1500 and 2000g (Table 4).
Efficacy of clinically indicated cerclage on neonatal outcomes in the propensity matched patients.
| Neonatal outcomes | OR* | 95% CI |
|---|---|---|
| Neonatal survival | 3.19 | 0.83-12.3 |
| Significant neonatal morbidity | 0.15 | 0.04-0.54 |
| Birth weight greater than 1500g | 9 | 2.80-28.96 |
| Birth weight greater than 2000g | 9.95 | 2.08-47.51 |
| Preterm birth more than 28 weeks | 7.43 | 2.72-20.26 |
| Preterm birth more than 32 weeks | 10.52 | 2.40-46.14 |
| Preterm birth more than 34 weeks | 21 | 2.56-172.30 |
OR, odds ratio; CI, confidence interval, obtained by GEE analysis
* Expectant management group is the reference group for all models.
Significant neonatal morbidity: respiratory distress syndrome which needs administration of surfactant, sepsis, intracranial hemorrhage, necrotizing enterocolitis, and bronchopulmonary dysplasia.
Discussion
Infants born preterm are at greater risk than infants born at term for mortality and a variety of health and developmental problems. The birth of a preterm infant can also bring considerable emotional and economic costs to families and have implications for public-sector services, such as health insurance, educational, and other social support systems.
The current methods for the diagnosis and treatment of preterm labor are currently based on an inadequate literature, and little is known about how preterm birth can be prevented. Treatment has been focused on inhibiting contractions. This has not reduced the incidence of preterm birth but has delayed delivery long enough to allow the administration of antenatal steroids and transfer of the mother and fetus to a hospital where they may receive appropriate care. These interventions have reduced the rates of perinatal mortality and morbidity. Although improvements in perinatal and neonatal care have significantly improved the rates of survival for infants born preterm, these infants remain at risk for a host of acute and chronic health problems.
Therapies and interventions for the prediction and the prevention of preterm birth are thus needed.
The management of a patient with second-trimester cervical dilation continues to pose a difficult dilemma for obstetricians. Management options considered include expectant management, cervical cerclage, and pregnancy termination via induction of labor or dilation and evacuation. In one large randomized clinical trial, the cerclage in women with a short cervix identified by routine sonographic screening at midtrimester has not substantially reduced the risk of preterm delivery (13). However, the women with cervical dilation were excluded in this trial. Based on the previous reports, it seems that cerclage placement does not improve pregnancy outcome in low-risk women with incidental detection of short cervix in the early second trimester (14,15).
However, when a physician identifies a dilated cervix by digital examination in high risk women, or in women with short cervix by transvaginal ultrasonography, there is still lack of evidence about cerclage or expectant management. Only one small randomized controlled trial of women with cervical dilation have all reported a reduction in preterm birth associated with cerclage in women with a dilated cervix when compared with bed rest (3). Recent retrospective cohort studies support that the physical examination-indicated cerclage has shown some benefits in selected women with cervical dilation less than 26 0/7 weeks (4, 16-18). In these previous studies, all women at all institutions were not screened for cervical dilation. Instead, women with cervical dilation were identified in 1 of 2 ways: 1) those found to have a shortened cervix or suspected cervical dilation on ultrasound or 2) those identified by screening digital examination performed because of a history of prior second-trimester loss, history of preterm birth, or subjective complaints of pressure or discharge. We identified candidate women with same methods. However, we included women with cervical dilation between 140/7 and 296/7 weeks' gestation.
The greatest risk of mortality and morbidity is for those infants born at the earliest gestational ages. However, those infants born nearer to term represent the greatest number of infants born preterm and also experience more complications than infants born at term. Even late preterm births (34 0/7-36 6/7 weeks), compared with term delivery, have been reported that it is associated with increased risk of respiratory distress syndrome and other respiratory morbidity (19). Other recent reports also demonstrated that late prematurity is associated with significant neonatal morbidity such as respiratory distress syndrome, intraventricular hemorrhage, and sepsis in cases of spontaneous low-risk singleton deliveries (20, 21). In our study, the average weeks of pregnancy prolongation in the expectant group was just 2.9 weeks, compared to 10.6 weeks in the cerclage group. Even though there was no difference in neonatal survival between two groups, significant neonatal morbidities were much less in the cerclage group. It might be a reason that 95% and 100% of women who were expectantly managed, compared with 47.5% and 65% women who received a cerclage, delivered prior to 34 weeks and 37 weeks.
Our study has several limitations. We evaluated observational data, and therefore the treatment strategy was not based on randomized assignment. The choice of cerclage was at the discretion of the treating physician or the patient. We acknowledge, however, that the particulars of clinical practice in the hospitals in this trial, as well as the specific experts in maternal fetal medicine who performed the procedures, may differ from those of other institutions and practitioners, potentially limiting the reproducibility of these results in other settings. The retrospective nature opens these data to bias. To minimize these biases, we used propensity-score matching, even though our sample size was decreased after the matching (9, 10).
Previous research has suggested that matching according to the propensity score eliminates a greater proportion of baseline differences between two treatments than does stratification or covariate adjustment (22). Given these issues and the findings of our study, we believe that a randomized trial of digital examination-indicated as compared with expectant management is warranted in patients between 14 0/7 and 29 6/7 weeks' gestation with painless cervical dilation between 1 and 4 cm.
In conclusion, this study supports digital examination-indicated cerclage in women who found to have a shortened cervix or suspected cervical dilation on ultrasound or who was identified by screening digital examination performed because of a history of prior second-trimester loss, history of preterm birth, or subjective complaints of pressure or discharge, between 14 0/7 and 29 6/7 weeks' gestation with painless cervical dilation between 1 and 4 cm, before the result of randomized trial is available. Even though we could not observe the significant improvement in neonatal survival, we found significant improvement in neonatal morbidity. It digital examination-indicated cerclage appears to prolong gestation, which might decrease significant neonatal morbidities.
Conflict of Interest
We have no conflicts of interest to declare.
References
1. Smith LK, Draper ES, Manktelow BN, Dorling JS, Field DJ. Socioeconomic inequalities in very preterm birth rates. Arch Dis Child Fetal Neonatal Ed. 2007;92:F11-4
2. Berghella V, Prasertcharoensuk W, Cotter A, Rasanen J, Mittal S, Chaithongwongwatthana S. et al. Does indomethacin prevent preterm birth in women with cervical dilatation in the second trimester? Am J Perinatol. 2009;26(1):13-9
3. Althuisius SM, Dekker GA, Hummel P, van Geijn HP. Cervical incompetence prevention randomized cerclage trial: emergency cerclage with bed rest versus bed rest alone. Am J Obstet Gynecol. 2003;189:907-10
4. Pereira L, Cotter A, Gómez R, Berghella V, Prasertcharoensuk W, Rasanen J. et al. Expectant management compared with physical examination-indicated cerclage (EM-PEC) in selected women with a dilated cervix at 14(0/7)-25(6/7) weeks: results from the EM-PEC international cohort study. Am J Obstet Gynecol. 2007;197(5):483.e1-8
5. Stevenson DK, Wright LL, Lemons JA, Oh W, Korones SB, Papile LA. et al. Very low birth weight outcomes of the National Institute of Child Health and Human Development Neonatal Research Network, January 1993 through December 1994. Am J Obstet Gynecol. 1998;179:1632-9
6. Bottoms SF, Paul RH, Mercer BM, MacPherson CA, Caritis SN, Moawad AH. et al. Obstetric determinants of neonatal survival: antenatal predictors of neonatal survival and morbidity in extremely low birth weight infants. Am J Obstet Gynecol. 1999;180:665-9
7. Behrman RE, Butler AS. Institute of Medicine (US) Committee on Understanding Premature Birth and Assuring Healthy Outcomes; Preterm Birth: Causes, Consequences, and Prevention. Washington, DC: National Academies Press. 2007
8. Gibbs R, Blanco J, St Clair P, Castaneda Y. Quantitative bacteriology of amniotic fluid from women with clinical intra-amniotic infection at term. J Infect Dis. 1982;145:1-8
9. Rosenbaum PR, Rubin DB. The central role of the propensity score in observational studies for causal effects. Biometrika. 1983;70:41-55
10. D'Agostino RB Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat Med. 1998;17:2265-81
11. Therneau TM, Grambsch PM. Modeling survival data: extending the Cox model. New York: Springer-Verlag. 2000
12. Klein JP, Moeschberger ML. Survival analysis: techniques for censored and truncated data. New York: Springer-Verlag. 1997
13. To MS, Alfirevic Z, Heath VC, Cicero S, Cacho AM, Williamson PR. et al. Fetal Medicine Foundation Second Trimester Screening Group. Cervical cerclage for prevention of preterm delivery in women with short cervix: randomised controlled trial. Lancet. 2004;363:1849-53
14. Berghella V, Odibo AO, Tolosa JE. Cerclage for prevention of preterm birth in women with a short cervix found on transvaginal ultrasound examination: a randomized trial. Am J Obstet Gynecol. 2004;191:1311-17
15. Incerti M, Ghidini A, Locatelli A, Poggi SH, Pezzullo JC. Cervical length 25 mm in low-risk women: a case control study of cerclage with rest vs rest alone. Am J Obstet Gynecol. 2007;197:315.e1-4
16. Daskalakis G, Papantoniou N, Mesogitis S, Antsaklis A. Management of cervical insufficiency and bulging fetal membranes. Obstet Gynecol. 2006;107:221-226
17. J.H. Stupin, David M, Siedentopf JP, Dudenhausen JW. Emergency cerclage versus bed rest for amniotic sac prolapse before 27 gestational weeks. Eur J Obstet Gynecol Reprod Biol. 2008;139:32-7
18. Ventolini G, Genrich TJ, Roth J, Neiger R. Pregnancy outcome after placement of 'rescue' Shirodkar cerclage. J Perinatol. 2009;29:276-9
19. Consortium on Safe Labor, Hibbard JU, Wilkins I, Sun L, Gregory K, Haberman S. et al. Respiratory morbidity in late preterm births. JAMA. 2010;304(4):419-25
20. McIntire DD, Leveno KJ. Neonatal mortality and morbidity rates in late preterm births compared with births at term. Obstet Gynecol. 2008;111(1):35-41
21. Melamed N, Klinger G, Tenenbaum-Gavish K, Herscovici T, Linder N, Hod M. et al. Short-term neonatal outcome in low-risk, spontaneous, singleton, late preterm deliveries. Obstet Gynecol. 2009;114(2 Pt 1):253-260
22. Austin PC, Mamdani MM. A comparison of propensity score methods: a case-study estimating the effectiveness of post-AMI statin use. Stat Med. 2006;25:2084-106
Author contact
![]() Corresponding author: Jong Chul Shin, Seoul St. Mary's Hospital, Department of Obstetrics and Gynecology, College of Medicine, Catholic University, Seoul, Korea. 505, Banpo-dong Seocho-gu, Seoul, 137-450, Korea. +82-2-2258-3021; +82-2--595-1549 (fax); jcshinac.kr
Corresponding author: Jong Chul Shin, Seoul St. Mary's Hospital, Department of Obstetrics and Gynecology, College of Medicine, Catholic University, Seoul, Korea. 505, Banpo-dong Seocho-gu, Seoul, 137-450, Korea. +82-2-2258-3021; +82-2--595-1549 (fax); jcshinac.kr